

Masked Uncontrolled Hypertension in CKD
- PMID: 26163421
- PMCID: PMC4769206
- DOI: 10.1681/ASN.2015030243
Masked Uncontrolled Hypertension in CKD
Abstract
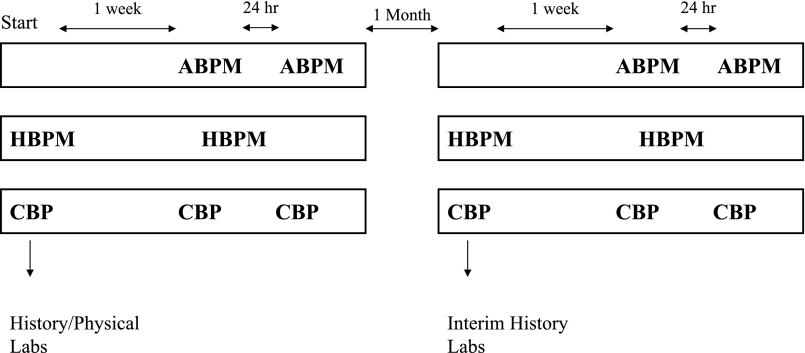
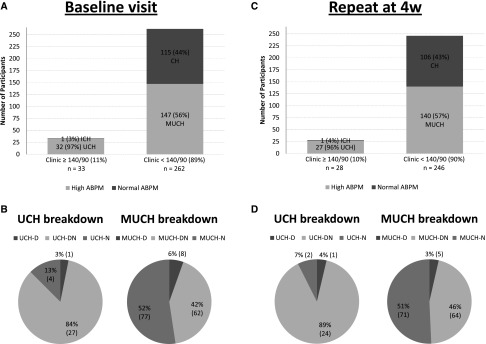
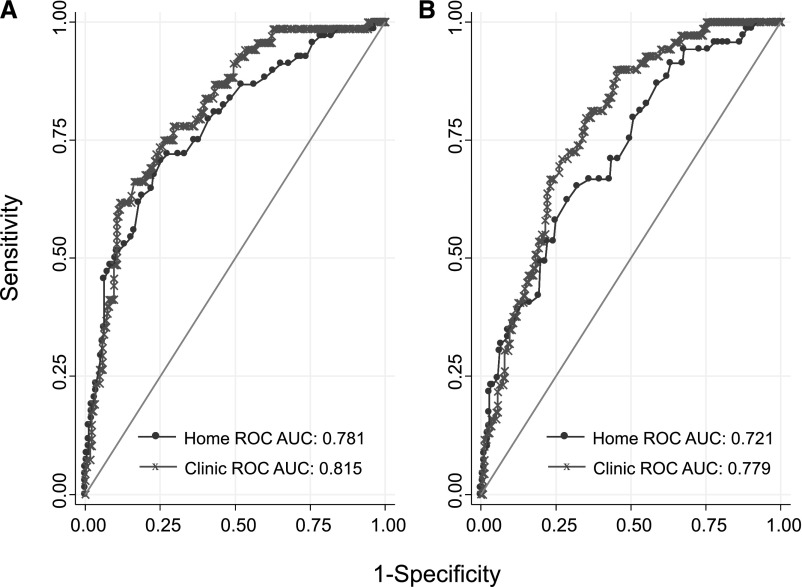
Masked uncontrolled hypertension (MUCH) is diagnosed in patients treated for hypertension who are normotensive in the clinic but hypertensive outside. In this study of 333 veterans with CKD, we prospectively evaluated the prevalence of MUCH as determined by ambulatory BP monitoring using three definitions of hypertension (daytime hypertension ≥135/85 mmHg; either nighttime hypertension ≥120/70 mmHg or daytime hypertension; and 24-hour hypertension ≥130/80 mmHg) or by home BP monitoring (hypertension ≥135/85 mmHg). The prevalence of MUCH was 26.7% by daytime ambulatory BP, 32.8% by 24-hour ambulatory BP, 56.1% by daytime or night-time ambulatory BP, and 50.8% by home BP. To assess the reproducibility of the diagnosis, we repeated these measurements after 4 weeks. Agreement in MUCH diagnosis by ambulatory BP was 75-78% (κ coefficient for agreement, 0.44-0.51), depending on the definition used. In contrast, home BP showed an agreement of only 63% and a κ coefficient of 0.25. Prevalence of MUCH increased with increasing clinic systolic BP: 2% in the 90-110 mmHg group, 17% in the 110-119 mmHg group, 34% in the 120-129 mmHg group, and 66% in the 130-139 mmHg group. Clinic BP was a good determinant of MUCH (receiver operating characteristic area under the curve 0.82; 95% confidence interval 0.76-0.87). In diagnosing MUCH, home BP was not different from clinic BP. In conclusion, among people with CKD, MUCH is common and reproducible, and should be suspected when clinic BP is in the prehypertensive range. Confirmation of MUCH diagnosis should rely on ambulatory BP monitoring.
Keywords: blood pressure; chronic kidney disease; hypertension.
Copyright © 2016 by the American Society of Nephrology.
Figures
References
-
- Coresh J, Astor BC, Greene T, Eknoyan G, Levey AS: Prevalence of chronic kidney disease and decreased kidney function in the adult US population: Third National Health and Nutrition Examination Survey. Am J Kidney Dis 41: 1–12, 2003 - PubMed
-
- Coresh J, Selvin E, Stevens LA, Manzi J, Kusek JW, Eggers P, Van Lente F, Levey AS: Prevalence of chronic kidney disease in the United States. JAMA 298: 2038–2047, 2007 - PubMed
-
- Coresh J, Wei GL, McQuillan G, Brancati FL, Levey AS, Jones C, Klag MJ: Prevalence of high blood pressure and elevated serum creatinine level in the United States: findings from the third National Health and Nutrition Examination Survey (1988–1994). Arch Intern Med 161: 1207–1216, 2001 - PubMed
-
- Klahr S, Levey AS, Beck GJ, Caggiula AW, Hunsicker L, Kusek JW, Striker G, Modification of Diet in Renal Disease Study Group : The effects of dietary protein restriction and blood-pressure control on the progression of chronic renal disease. N Engl J Med 330: 877–884, 1994 - PubMed
-
- Agodoa LY, Appel L, Bakris GL, Beck G, Bourgoignie J, Briggs JP, Charleston J, Cheek D, Cleveland W, Douglas JG, Douglas M, Dowie D, Faulkner M, Gabriel A, Gassman J, Greene T, Hall Y, Hebert L, Hiremath L, Jamerson K, Johnson CJ, Kopple J, Kusek J, Lash J, Lea J, Lewis JB, Lipkowitz M, Massry S, Middleton J, Miller ER, III, Norris K, O’Connor D, Ojo A, Phillips RA, Pogue V, Rahman M, Randall OS, Rostand S, Schulman G, Smith W, Thornley-Brown D, Tisher CC, Toto RD, Wright JT, Jr, Xu S, African American Study of Kidney Disease and Hypertension (AASK) Study Group : Effect of ramipril vs amlodipine on renal outcomes in hypertensive nephrosclerosis: a randomized controlled trial. JAMA 285: 2719–2728, 2001 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
