

Validation of a frailty index in patients undergoing curative surgery for urologic malignancy and comparison with other risk stratification tools
- PMID: 26163940
- PMCID: PMC4584178
- DOI: 10.1016/j.urolonc.2015.06.002
Validation of a frailty index in patients undergoing curative surgery for urologic malignancy and comparison with other risk stratification tools
Abstract
Objective: To retrospectively validate and compare a modified frailty index predicting adverse outcomes and other risk stratification tools among patients undergoing urologic oncological surgeries.
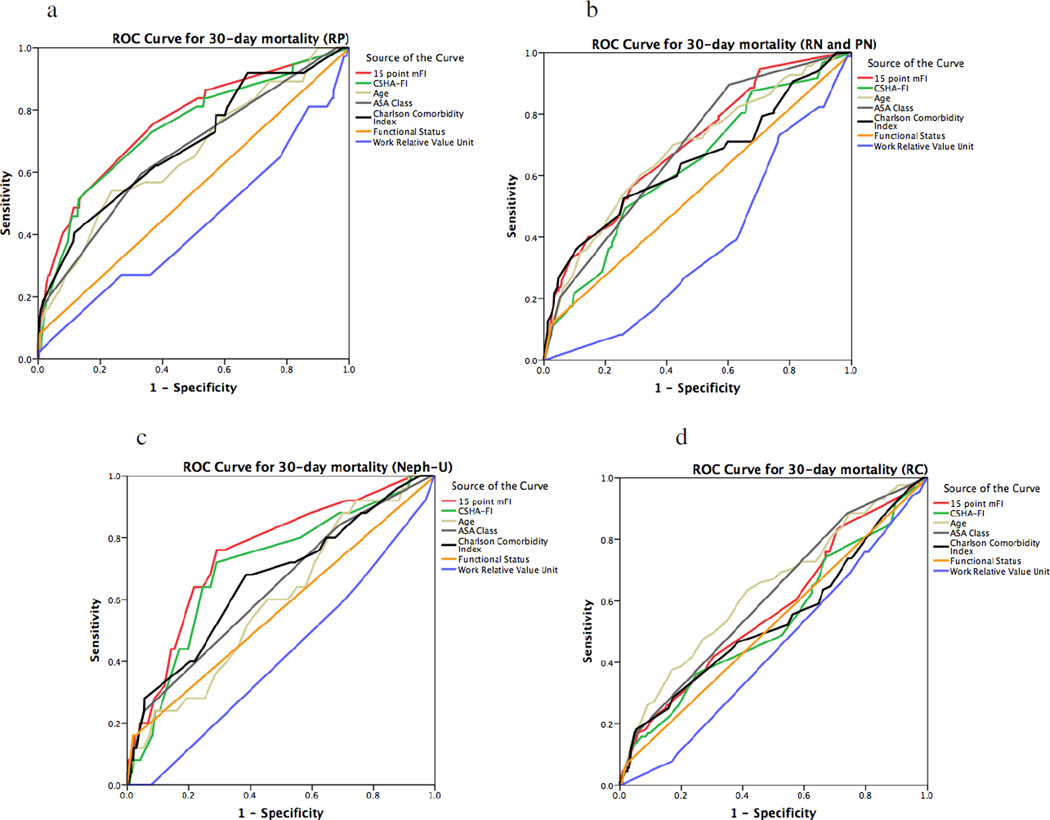
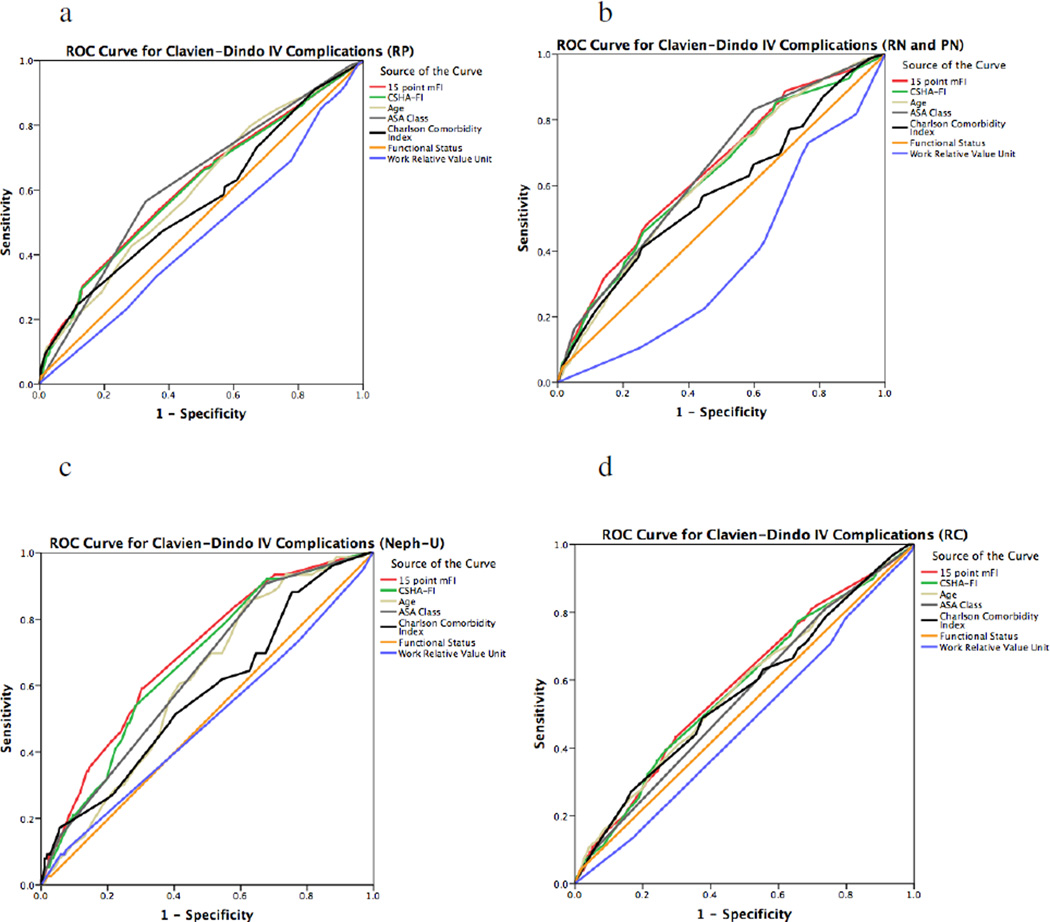
Materials and methods: The American College of Surgeons National Surgical Quality Improvement Program was queried from 2005 to 2013 to identify patients undergoing cystectomy, prostatectomy, nephrectomy, and nephroureterectomy. Using the Canadian Study of Health and Aging Frailty Index, 11 variables were matched to the database; 4 were also added because of their relevance in oncology patients. The incidence of mortality, Clavien-Dindo IV complications, and adverse events were assessed with patients grouped according to their modified frailty index score.
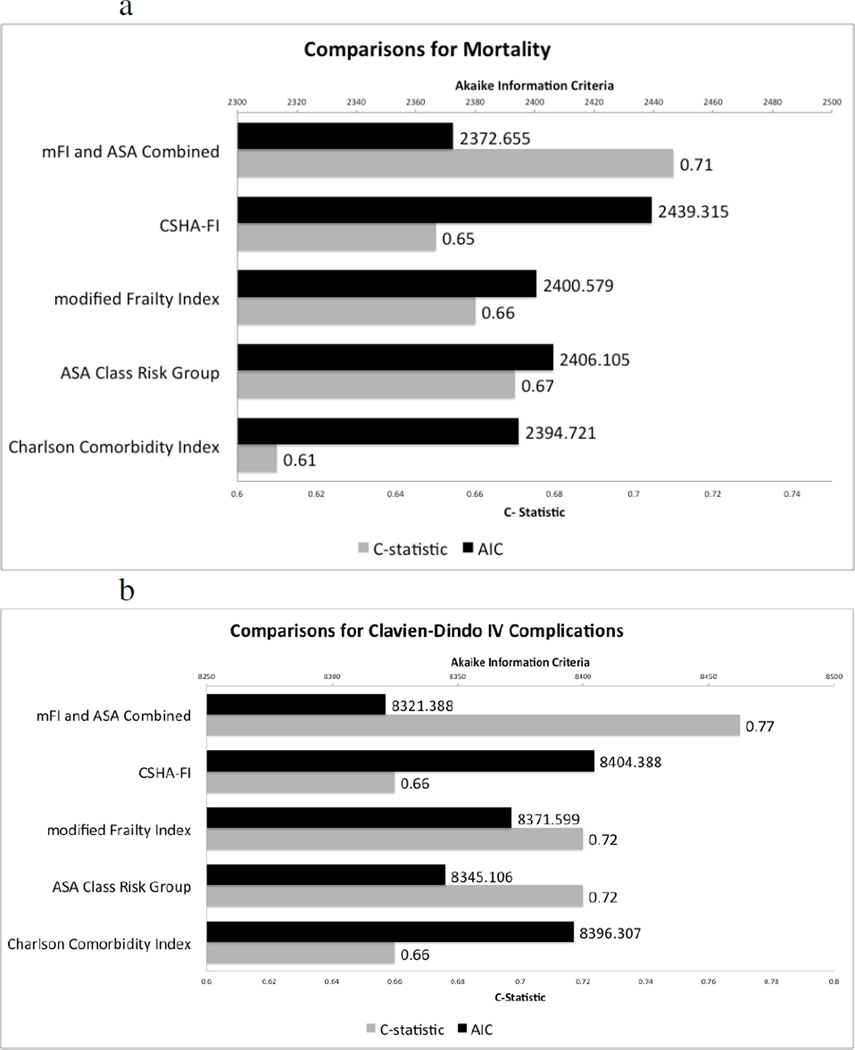
Results: We identified 41,681 patients who were undergoing surgery for presumed urologic malignancy. Patients with a high frailty index score of >0.20 had a 3.70 odds of a Clavien-Dindo IV event (CI: 2.865-4.788, P<0.0005) and a 5.95 odds of 30-day mortality (CI: 3.72-9.51, P<0.0005) in comparison with nonfrail patients after adjusting for race, sex, age, smoking history, and procedure. Using C-statistics to compare the sensitivity and specificity of the predictive ability of different models per risk stratification tool and the Akaike information criteria to assess for the fit of the models with the data, the modified frailty index was comparable or superior to the Charlson comorbidity index but inferior to the American Society of Anesthesiologists Risk Class in predicting 30-day mortality or Clavien-Dindo IV events. When the modified frailty index was augmented with the American Society of Anesthesiologists Risk Class, the new index was superior in all aspects in comparison to other risk stratification tools.
Conclusion: Existing risk stratification tools may be improved by incorporating variables in our 15-point modified frailty index as well as other factors such as walking speed, exhaustion, and sarcopenia to fully assess frailty. This is relevant in diseases such as kidney and prostate cancer, where surveillance and other nonsurgical interventions exist as alternatives to a potentially complicated surgery. In these scenarios, our modified frailty index augmented by the American Society of Anesthesiologists Risk Class may help inform which patients have increased surgical complications that may outweigh the benefit of surgery although this index needs prospective validation.
Keywords: Frail elderly; Patient survival; Preoperative evaluation; Surgical outcomes; Urologic oncology.
Copyright © 2015 Elsevier Inc. All rights reserved.
Figures
Comment in
-
Re: Validation of a Frailty Index in Patients Undergoing Curative Surgery for Urologic Malignancy and Comparison with Other Risk Stratification Tools.J Urol. 2016 Sep;196(3):788-90. doi: 10.1016/j.juro.2016.06.038. Epub 2016 Jun 16. J Urol. 2016. PMID: 27597080 No abstract available.
References
-
- Fried LP. Frailty in older adults: Evidence for a phenotype. The journals of gerontology Series A. Biological sciences and medical sciences. 2001;56(3) - PubMed
-
- Handforth C, Clegg A, Young C, Simpkins S, Seymour MT, Selby PJ, et al. The prevalence and outcomes of frailty in older cancer patients: a systematic review. Annals of oncology : official journal of the European Society for Medical Oncology / ESMO. 2014 Nov 17; PubMed PMID: 25403592. - PubMed
-
- Rockwood K, Song X, MacKnight C, Bergman H, Hogan DB, McDowell I, et al. A global clinical measure of fitness and frailty in elderly people. CMAJ : Canadian Medical Association journal = journal de l'Association medicale canadienne. 2005 Aug 30;173(5):489–495. PubMed PMID: 16129869. Pubmed Central PMCID: 1188185. - PMC - PubMed
-
- Rockwood K, Andrew M, Mitnitski A. A comparison of two approaches to measuring frailty in elderly people. J Gerontol a-Biol. 2007 Jul;62(7):738–743. PubMed PMID: WOS:000253828700008. English. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
