

Equating Visual Function Scales to Facilitate Reporting of Medicare Functional G-Code Severity/Complexity Modifiers for Low-Vision Patients
- PMID: 26163943
- PMCID: PMC4601936
- DOI: 10.1016/j.apmr.2015.06.013
Equating Visual Function Scales to Facilitate Reporting of Medicare Functional G-Code Severity/Complexity Modifiers for Low-Vision Patients
Abstract
Objective: To present a method of estimating and equating scales across functional assessment instruments that appropriately represents changes in a patient's functional ability and can be meaningfully mapped to changes in Medicare G-code severity modifiers.
Design: Previously published measures of patients' overall visual ability, estimated from low-vision patient responses to 7 different visual function rating scale questionnaires, are equated and mapped onto Medicare G-code severity modifiers.
Setting: Outpatient low-vision rehabilitation clinics.
Participants: The analyses presented in this article were performed on raw or summarized low-vision patient ratings of visual function questionnaire (VFQ) items obtained from previously published research studies.
Interventions: Previously published visual ability measures from Rasch analysis of low-vision patient ratings of items in different VFQs (National Eye Institute Visual Functioning Questionnaire, Index of Visual Functioning, Activities of Daily Vision Scale, Visual Activities Questionnaire) were equated with the Activity Inventory (AI) scale. The 39 items in the Self-Report Assessment of Functional Visual Performance (SRAFVP) and the 48 items in the Veterans Affairs Low Vision Visual Functioning Questionnaire (VA LV VFQ) were paired with similar items in the AI in order to equate the scales.
Main outcome measures: Tests using different observation methods and indicators cannot be directly compared on the same scale. All test results would have to be transformed to measures of the same functional ability variable on a common scale as described here, before a single measure could be estimated from the multiple measures.
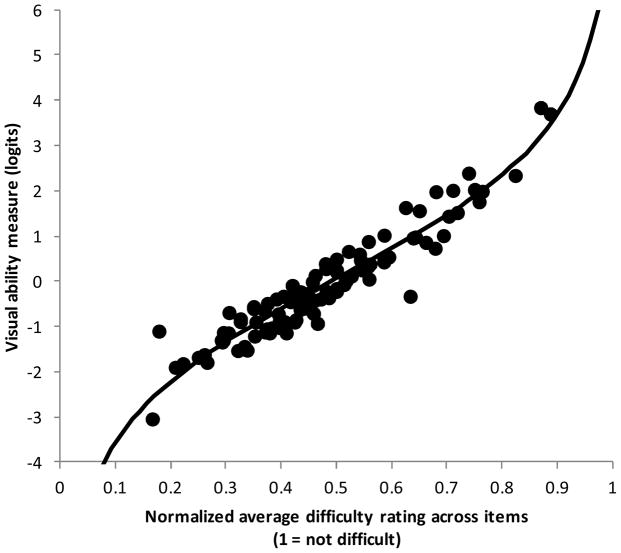
Results: Bivariate regression analysis was performed to linearly transform the SRAFVP and VA LV VFQ item measures to the AI item measure scale. The nonlinear relationship between person measures of visual ability on a logit scale and item response raw scores was approximated with a logistic function, and the 2 regression coefficients were estimated for each of the 7 VFQs. These coefficients can be used with the logistic function to estimate functional ability on the same interval scale for each VFQ and for transforming raw VFQ responses to Medicare's G-code severity modifier categories.
Conclusions: The principle of using equated interval scales allows for comparison across measurement instruments of low-vision functional status and outcomes, but can be applied to any area of rehabilitation.
Keywords: Medicare; Occupational therapy; Outcome assessment (health care); Rehabilitation; Vision, low.
Copyright © 2015 American Congress of Rehabilitation Medicine. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of Interest: Dr. Robert Massof was a consultant to Alcon
Figures




References
-
- [Accessed 14 Jan 2015];American Academy of Ophthalmology Preferred Practice Patterns Vision Rehabilitation. http://one.aao.org/preferred-practice-pattern/vision-rehabilitation-ppp-....
-
- Centers for Medicare and Medicaid Services, US Department of Health and Human Services. Program memorandum: intermediaries/carriers: provider education article: Medicare coverage of rehabilitation services for beneficiaries with vision impairment. 2002 May 29; Transmittal AB-02-078. Also available: http://www.cms.gov/Regulations-and-Guidance/Guidance/Transmittals/Downlo....
-
-
MLN Matters MM 8005 (Revised) Related to CR 8005 and Transmittals R165BP, R2622CP: Implementing the Claims-Based Data Collection Requirement for Outpatient Therapy Services – Section 3005 (g) of the Middle Class Tax Relief and Jobs Creation Act (MCTRJCA) of 2012. Also available:
http://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNMattersArticles/Downloads/MM8005.pdf
-
-
- Mediware. [Last accessed 31 January, 2015]; website: http://www.mediware.com/rehabilitation/tools/item/g-code-conversion-calc....
-
- Velozo CA, Warren M, Hicks E, Berger KA. Generating clinical outputs for self-reports of visual functioning. Optom Vis Sci. 2013 Aug;90(8):765–75. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources

