

Cardiomyopathy Phenotypes and Outcomes for Children With Left Ventricular Myocardial Noncompaction: Results From the Pediatric Cardiomyopathy Registry
- PMID: 26164213
- PMCID: PMC4630116
- DOI: 10.1016/j.cardfail.2015.06.381
Cardiomyopathy Phenotypes and Outcomes for Children With Left Ventricular Myocardial Noncompaction: Results From the Pediatric Cardiomyopathy Registry
Abstract
Background: Left ventricular noncompaction (LVNC) is a distinct form of cardiomyopathy characterized by hypertrabeculation of the left ventricle. The LVNC phenotype may occur in isolation or with other cardiomyopathy phenotypes. Prognosis is incompletely characterized in children.
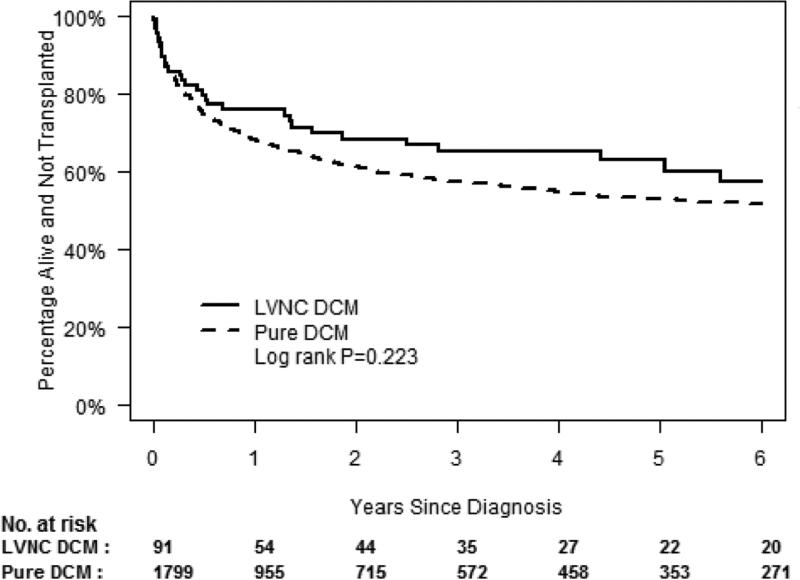
Methods and results: According to diagnoses from the National Heart, Lung, and Blood Institute-funded Pediatric Cardiomyopathy Registry from 1990 to 2008, 155 of 3,219 children (4.8%) had LVNC. Each LVNC patient was also classified as having an associated echocardiographically diagnosed cardiomyopathy phenotype: dilated (DCM), hypertrophic (HCM), restrictive (RCM), isolated, or indeterminate. The time to death or transplantation differed among the phenotypic groups (P = .035). Time to listing for cardiac transplantation significantly differed by phenotype (P < .001), as did time to transplantation (P = .015). The hazard ratio for death/transplantation (with isolated LVNC as the reference group) was 4.26 (95% confidence interval [CI] 0.78-23.3) for HCM, 6.35 (95% CI 1.52-26.6) for DCM, and 5.66 (95% CI 1.04-30.9) for the indeterminate phenotype. Most events occurred in the 1st year after diagnosis.
Conclusions: LVNC is present in at least 5% of children with cardiomyopathy. The specific LVNC-associated cardiomyopathy phenotype predicts the risk of death or transplantation and should inform clinical management.
Keywords: Cardiomyopathy; heart failure; pediatrics.
Copyright © 2015 Elsevier Inc. All rights reserved.
Figures





References
-
- Maron BJ, Towbin JA, Thiene G, Antzelevitch C, Corrado D, Arnett D, et al. Contemporary definitions and classification of the cardiomyopathies: an American Heart Association Scientific Statement from the Council on Clinical Cardiology, Heart Failure and Transplantation Committee; Quality of Care and Outcomes Research and Functional Genomics and Translational Biology Interdisciplinary Working Groups; and Council on Epidemiology and Prevention. Circulation. 2006;113:1807–16. - PubMed
-
- Richardson P, McKenna W, Bristow M, Maisch B, Mautner B, O'Connell J, et al. Report of the 1995 World Health Organization/International Society and Federation of Cardiology Task Force on the Definition and Classification of Cardiomyopathies. Circulation. 1996;93:841–2. - PubMed
-
- Tigen K, Karaahmet T, Gurel E, Cevik C, Basaran Y. Biventricular noncompaction: a case report. Echocardiography. 2008;25:993–6. - PubMed
-
- Sarma RJ, Chana A, Elkayam Left ventricular noncompaction. Prog Cardiovasc Dis. 2010;52:264–73. - PubMed
-
- Dusek J, Ostadal B, Duskova M. Postnatal persistence of spongy myocardium with embryonic blood supply. Arch Pathol. 1975;99:312–7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
