

Covert and Overt Hepatic Encephalopathy: Diagnosis and Management
- PMID: 26164219
- PMCID: PMC4618040
- DOI: 10.1016/j.cgh.2015.06.039
Covert and Overt Hepatic Encephalopathy: Diagnosis and Management
Abstract
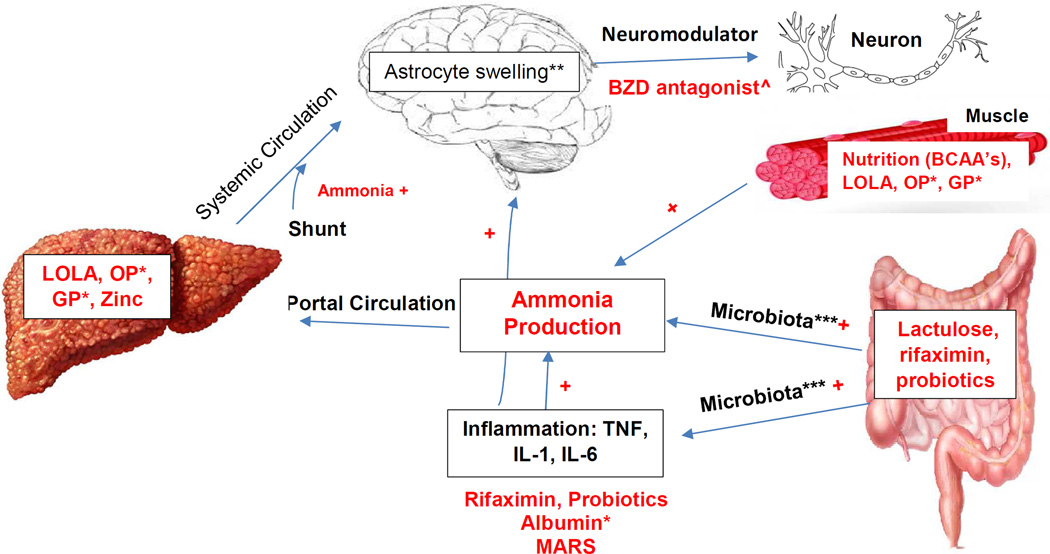
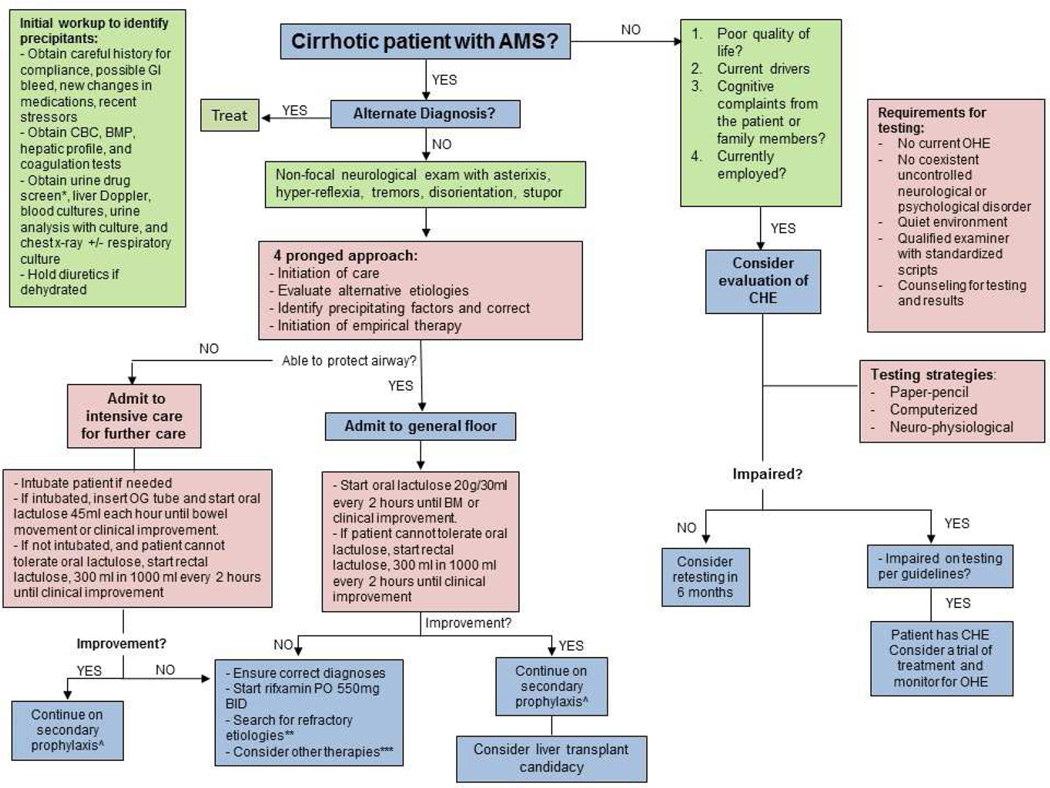
Hepatic encephalopathy (HE) is part of a spectrum of neurocognitive changes in cirrhosis. HE is divided into 2 broad categories based on severity: covert hepatic encephalopathy (CHE) and overt hepatic encephalopathy (OHE). CHE has a significant impact on a patient's quality of life, driving performance, and recently has been associated with increased hospitalizations and death. Likewise, OHE is associated with increased rates of hospitalizations and mortality, and poor quality of life. Given its significant burden on patients, care takers, and the health care system, early diagnosis and management are imperative. In addition, focus also should be directed on patient and family member education on the disease progression and adherence to medications. Treatment strategies include the use of nonabsorbable disaccharides, antibiotics (ie, rifaximin), and, potentially, probiotics. Other therapies currently under further investigation include L-ornithine-L-aspartate, ornithine phenylacetate, glycerol phenylbutyrate, molecular adsorbent recirculating system, and albumin infusion.
Keywords: Ammonia; Cirrhosis; Covert Hepatic Encephalopathy; Hepatic Encephalopathy; Lactulose; Overt Hepatic Encephalopathy; Rifaximin.
Copyright © 2015 AGA Institute. Published by Elsevier Inc. All rights reserved.
Figures
Similar articles
-
Management of hepatic encephalopathy in the hospital.Mayo Clin Proc. 2014 Feb;89(2):241-53. doi: 10.1016/j.mayocp.2013.11.009. Epub 2014 Jan 8. Mayo Clin Proc. 2014. PMID: 24411831 Free PMC article. Review.
-
Overt Hepatic Encephalopathy: Current Pharmacologic Treatments and Improving Clinical Outcomes.Am J Med. 2021 Nov;134(11):1330-1338. doi: 10.1016/j.amjmed.2021.06.007. Epub 2021 Jul 7. Am J Med. 2021. PMID: 34242619 Review.
-
Hepatic encephalopathy: how to test and treat.Curr Opin Gastroenterol. 2014 May;30(3):265-71. doi: 10.1097/MOG.0000000000000066. Curr Opin Gastroenterol. 2014. PMID: 24717765 Review.
-
Hepatic Encephalopathy: Diagnostic Tools and Management Strategies.Med Clin North Am. 2023 May;107(3):517-531. doi: 10.1016/j.mcna.2023.01.003. Epub 2023 Feb 20. Med Clin North Am. 2023. PMID: 37001951 Review.
-
Should We Treat Minimal/Covert Hepatic Encephalopathy, and with What?Clin Liver Dis. 2015 Aug;19(3):487-95. doi: 10.1016/j.cld.2015.04.002. Epub 2015 May 19. Clin Liver Dis. 2015. PMID: 26195203 Review.
Cited by
-
The Management of Hepatic Encephalopathy from Ward to Domiciliary Care: Current Evidence and Gray Areas.J Clin Med. 2023 Dec 27;13(1):166. doi: 10.3390/jcm13010166. J Clin Med. 2023. PMID: 38202173 Free PMC article. Review.
-
Novel Insights Into Pathogenesis and Therapeutic Strategies of Hepatic Encephalopathy, From the Gut Microbiota Perspective.Front Cell Infect Microbiol. 2021 Feb 22;11:586427. doi: 10.3389/fcimb.2021.586427. eCollection 2021. Front Cell Infect Microbiol. 2021. PMID: 33692964 Free PMC article. Review.
-
Bile duct ligation differently regulates protein expressions of organic cation transporters in intestine, liver and kidney of rats through activation of farnesoid X receptor by cholate and bilirubin.Acta Pharm Sin B. 2023 Jan;13(1):227-245. doi: 10.1016/j.apsb.2022.06.010. Epub 2022 Jun 16. Acta Pharm Sin B. 2023. PMID: 36815051 Free PMC article.
-
Acute care and emergency general surgery in patients with chronic liver disease: how can we optimize perioperative care? A review of the literature.World J Emerg Surg. 2018 Jul 18;13:32. doi: 10.1186/s13017-018-0194-1. eCollection 2018. World J Emerg Surg. 2018. PMID: 30034510 Free PMC article. Review.
-
Validation of the Korean Stroop Test in Diagnosis of Minimal Hepatic Encephalopathy.Sci Rep. 2019 May 29;9(1):8027. doi: 10.1038/s41598-019-44503-w. Sci Rep. 2019. PMID: 31142824 Free PMC article.
References
-
- Bustamante J, Rimola A, Ventura PJ, et al. Prognostic significance of hepatic encephalopathy in patients with cirrhosis. J Hepatol. 1999;30:890–895. - PubMed
-
- Ferenci P, Lockwood A, Mullen K, et al. Hepatic encephalopathy--definition, nomenclature, diagnosis, and quantification: final report of the working party at the 11th World Congresses of Gastroenterology, Vienna, 1998. Hepatology. 2002;35:716–721. - PubMed
-
- Vilstrup H, Amodio P, Bajaj J, et al. Hepatic encephalopathy in chronic liver disease: 2014 Practice Guideline by the American Association for the Study of Liver Diseases and the European Association for the Study of the Liver. Hepatology. 2014;60:715–735. - PubMed
-
- Bajaj JS, Wade JB, Sanyal AJ. Spectrum of neurocognitive impairment in cirrhosis: Implications for the assessment of hepatic encephalopathy. Hepatology. 2009;50:2014–2021. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
