

Out-of-pocket health expenditures and antimicrobial resistance in low-income and middle-income countries: an economic analysis
- PMID: 26164481
- PMCID: PMC4609169
- DOI: 10.1016/S1473-3099(15)00149-8
Out-of-pocket health expenditures and antimicrobial resistance in low-income and middle-income countries: an economic analysis
Abstract
Introduction: The decreasing effectiveness of antimicrobial agents is a growing global public health concern. Low-income and middle-income countries are vulnerable to the loss of antimicrobial efficacy because of their high burden of infectious disease and the cost of treating resistant organisms. We aimed to assess if copayments in the public sector promoted the development of antibiotic resistance by inducing patients to purchase treatment from less well regulated private providers.
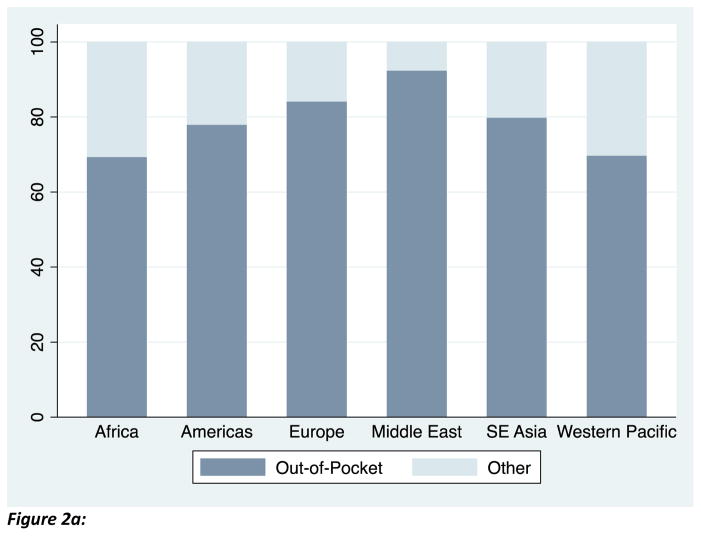
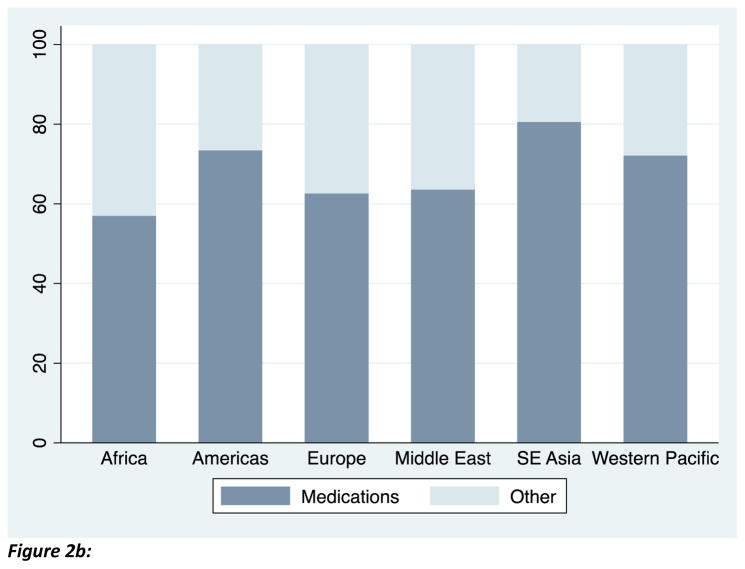
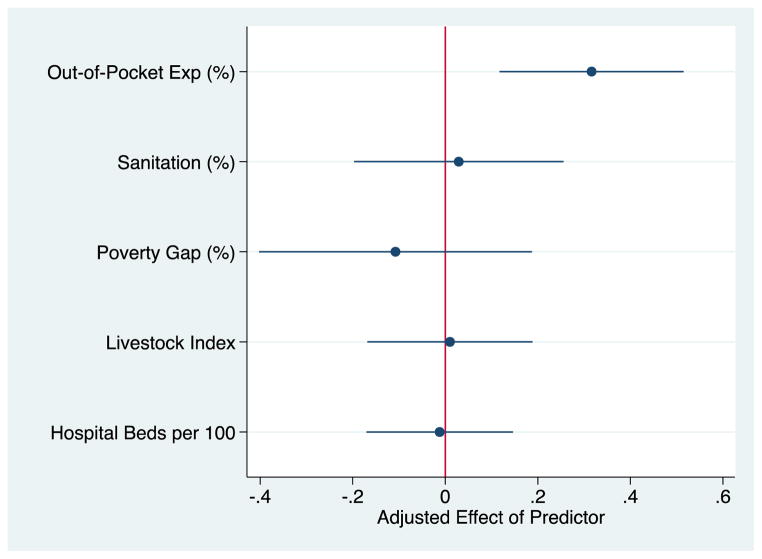
Methods: We analysed data from the WHO 2014 Antibacterial Resistance Global Surveillance report. We assessed the importance of out-of-pocket spending and copayment requirements for public sector drugs on the level of bacterial resistance in low-income and middle-income countries, using linear regression to adjust for environmental factors purported to be predictors of resistance, such as sanitation, animal husbandry, and poverty, and other structural components of the health sector. Our outcome variable of interest was the proportion of bacterial isolates tested that showed resistance to a class of antimicrobial agents. In particular, we computed the average proportion of isolates that showed antibiotic resistance for a given bacteria-antibacterial combination in a given country.
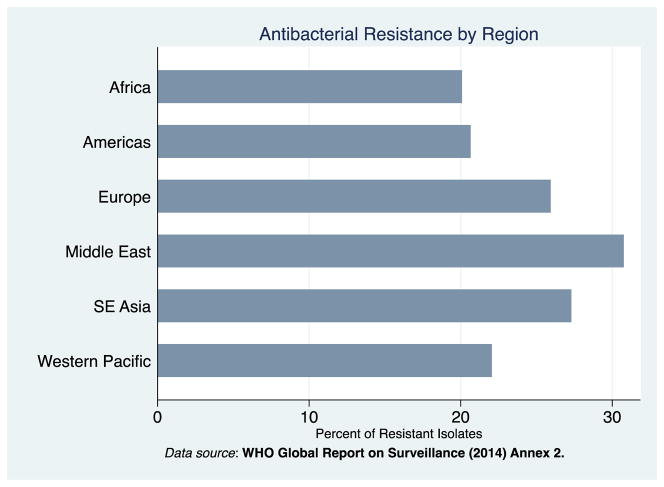
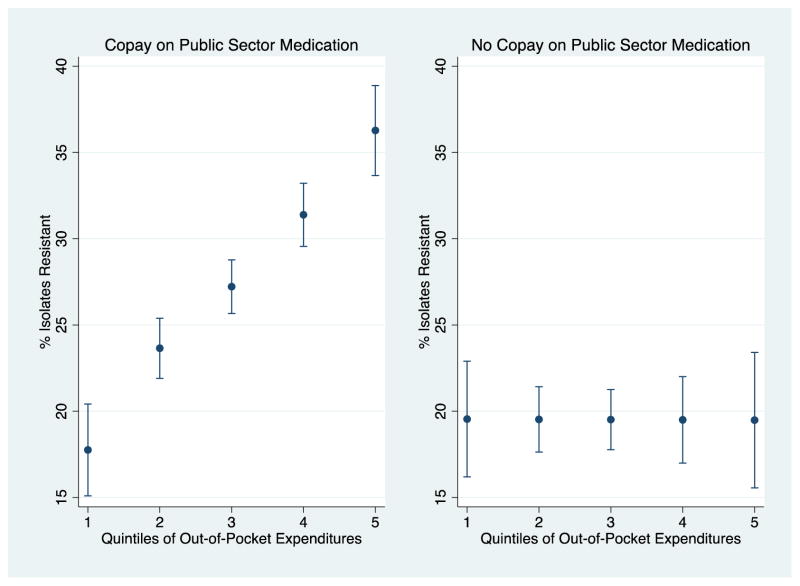
Findings: Our sample included 47 countries (23 in Africa, eight in the Americas, three in Europe, eight in the Middle East, three in southeast Asia, and two in the western Pacific). Out-of-pocket health expenditures were the only factor significantly associated with antimicrobial resistance. A ten point increase in the percentage of health expenditures that were out-of-pocket was associated with a 3·2 percentage point increase in resistant isolates (95% CI 1·17-5·15; p=0·002). This association was driven by countries requiring copayments for drugs in the public health sector. Of these countries, moving from the 20th to 80th percentile of out-of-pocket health expenditures was associated with an increase in resistant bacterial isolates from 17·76% (95% CI 12·54-22·97) to 36·27% (31·16-41·38).
Interpretation: Out-of-pocket health expenditures were strongly correlated with antimicrobial resistance in low-income and middle-income countries. This relation was driven by countries that require copayments on drugs in the public sector. Our data suggest cost-sharing of antimicrobials in the public sector might drive demand to the private sector in which supply-side incentives to overprescribe are probably heightened and quality assurance less standardised.
Funding: National Institutes of Health.
Copyright © 2015 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Figures
Comment in
-
Antibiotics, copayments, and antimicrobial resistance: investment matters.Lancet Infect Dis. 2015 Oct;15(10):1125-1127. doi: 10.1016/S1473-3099(15)00057-2. Epub 2015 Jul 9. Lancet Infect Dis. 2015. PMID: 26164480 No abstract available.
References
-
- World Health Organization. Antimicrobial resistance: global report on surveillance. 2014
-
- Wolkewitz M, Frank U, Philips G, Schumacher M, Davey P for the BURDEN Study Group. Mortality associated with in-hospital bacteremia caused by Staphylococcus aureus: a multistate analysis with follow-up beyond hospital discharge. J Antimicrob Chemother. 2011;66:381–386. - PubMed
-
- US Centers for Disease Control and Prevention. [accessed July 24, 2014];Antibiotic resistance threats in the United States 2013. 2013 Apr; http://www.cdc.gov/drugresistance/threat-report-2013/pdf/ar-threats-2013....
-
- Howard DH, Scott DR. The Economic Burden of Drug Resistance. Clinical Infectious Disease. 2005;41:S283–286. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
