

Initiation of antiretroviral therapy at high CD4+ cell counts is associated with positive treatment outcomes
- PMID: 26165354
- PMCID: PMC4573912
- DOI: 10.1097/QAD.0000000000000790
Initiation of antiretroviral therapy at high CD4+ cell counts is associated with positive treatment outcomes
Erratum in
- AIDS. 2016 Feb 20;30(4):677
Abstract
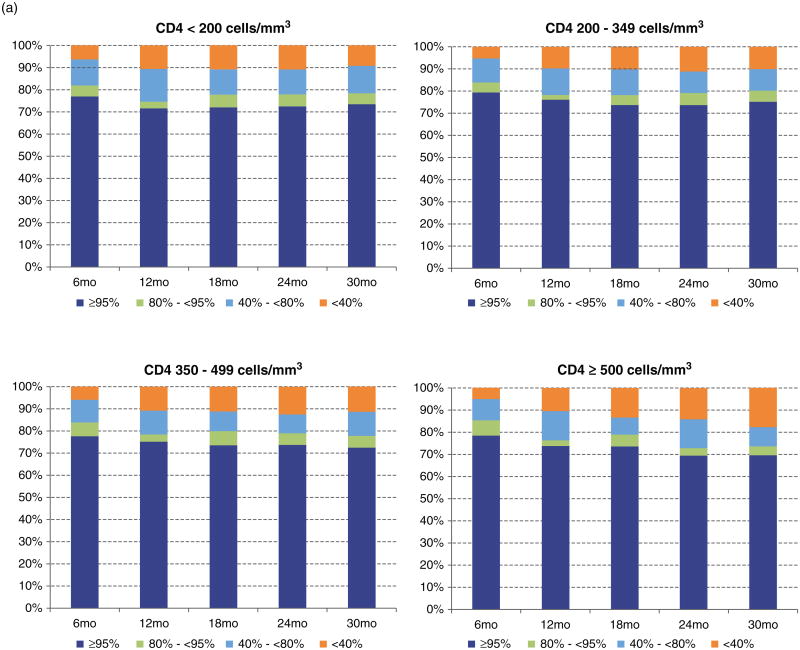
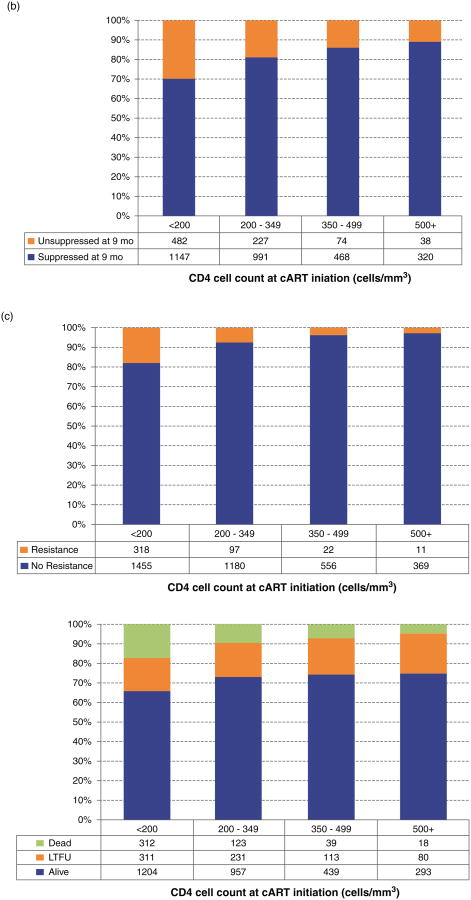
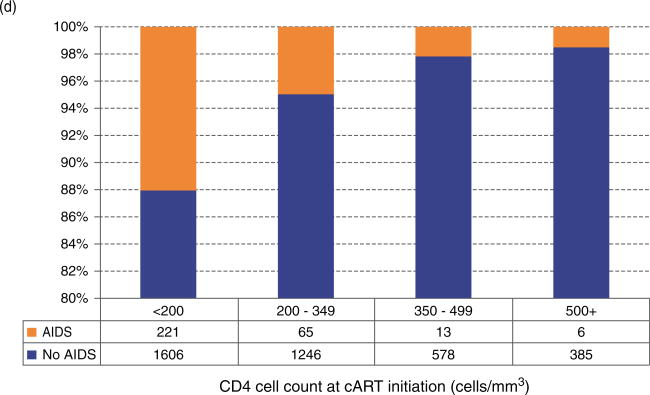
Objective: There is limited research investigating the possible mechanisms of how starting combination antiretroviral therapy (cART) at a higher CD4 cell count decreases mortality. This study investigated the association between initiating cART with short-term and long-term achievement of viral suppression; emergence of any drug resistance and of an AIDS-defining illness (ADI); long-term treatment adherence; and all-cause mortality.
Methods: This retrospective cohort study included 4120 naive patients who initiated cART between 2000 and 2012. Patients were followed until 2013, death or until the last contact date (varied by outcome). The main exposure was the interaction between period of cART initiation (2000-2006 and 2007-2012) and CD4 cell count at cART initiation (<500 versus ≥500 cells/μl). We considered both baseline and longitudinal covariates. We fitted different multivariable models using cross-sectional and longitudinal statistical methods, depending on the outcome.
Results: Patients who initiated cART with a CD4 cell count at least 500 cells/μl in 2007-2012 had an increased likelihood of achieving viral suppression at 9 months and of maintaining an adherence level of at least 95% over time, and the lowest probability of developing any resistance and an ADI during follow-up. These patients were not the ones with the highest likelihood of maintaining viral suppression over time, most likely due to viral load blips experienced during the follow-up.
Conclusion: The outcomes in this study likely play an important role in explaining the positive impact of early cART initiation on mortality. These results should alleviate some of the concerns clinicians may have when initiating cART in patients with high CD4s as recommended by current treatment guidelines.
Conflict of interest statement
Figures
References
-
- The Joint United Nations Programme on HIV/AIDS. HIV estimates with uncertainty bounds. 2014 http://www.unaids.org/en/resources/documents/2014/HIV_estimates_with_und....
-
- Molina JM, Cahn P, Grinsztejn B, Lazzarin A, Mills A, Saag M, et al. Rilpivirine versus efavirenz with tenofovir and emtricitabine in treatment-naive adults infected with HIV-1 (ECHO): a phase 3 randomised double-blind active-controlled trial. Lancet. 2011;378:238–246. - PubMed
-
- Nelson M, Amaya G, Clumeck N, Arns da Cunha C, Jayaweera D, Junod P, et al. Efficacy and safety of rilpivirine in treatment-naive, HIV-1-infected patients with hepatitis B virus/hepatitis C virus coinfection enrolled in the Phase III randomized, double-blind ECHO and THRIVE trials. J Antimicrob Chemother. 2012;67:2020–2028. - PMC - PubMed
-
- Raffi F, Jaeger H, Quiros-Roldan E, Albrecht H, Belonosova E, Gatell JM, et al. Once-daily dolutegravir versus twice-daily raltegravir in antiretroviral-naive adults with HIV-1 infection (SPRING-2 study): 96 week results from a randomised, double-blind, non-inferiority trial. Lancet Infect Dis. 2013;13:927–935. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
