

The Value of Palliative Gastrectomy for Gastric Cancer Patients With Intraoperatively Proven Peritoneal Seeding
- PMID: 26166075
- PMCID: PMC4504616
- DOI: 10.1097/MD.0000000000001051
The Value of Palliative Gastrectomy for Gastric Cancer Patients With Intraoperatively Proven Peritoneal Seeding
Abstract
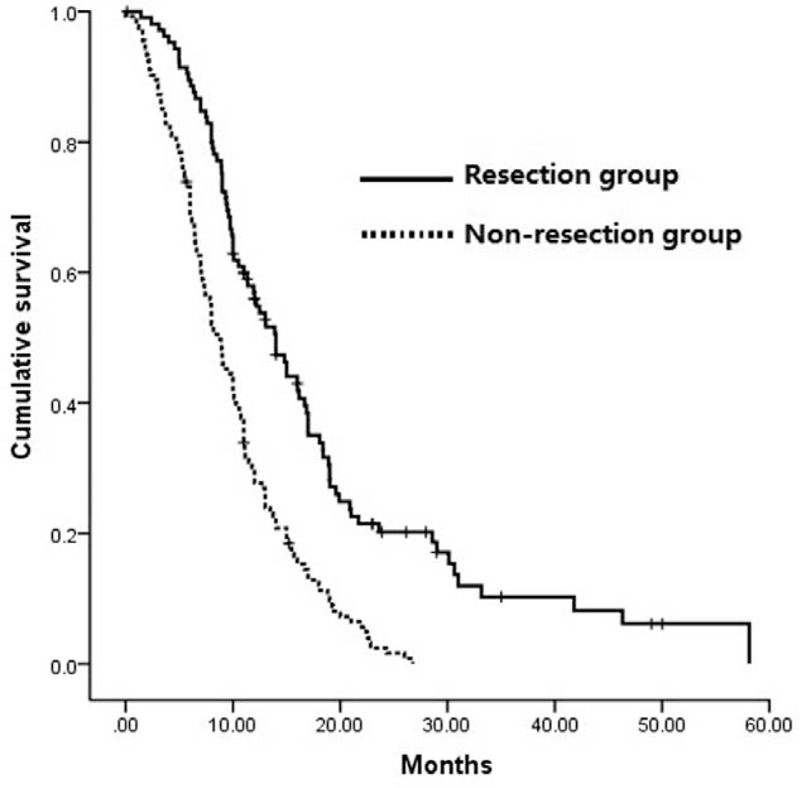
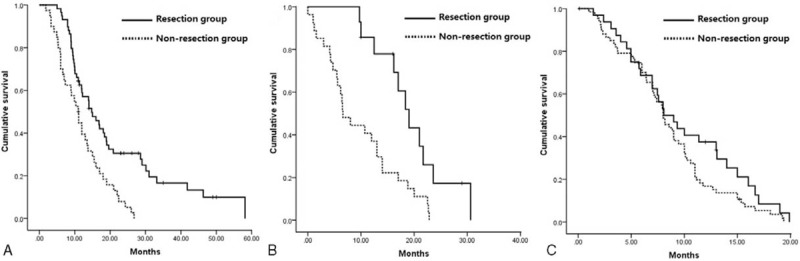
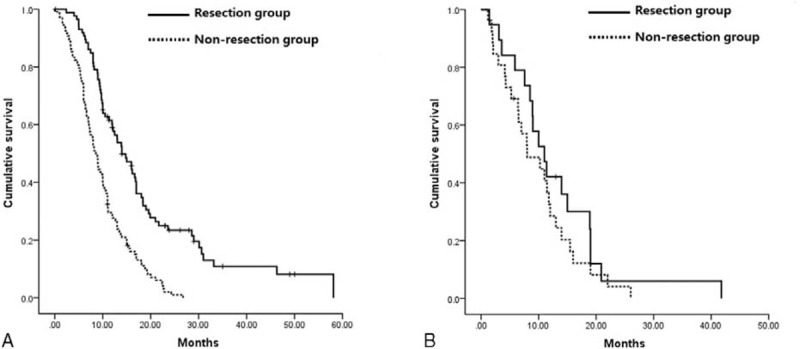
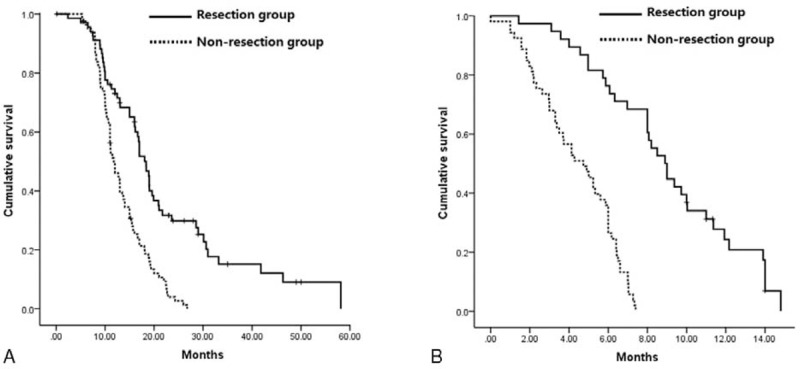
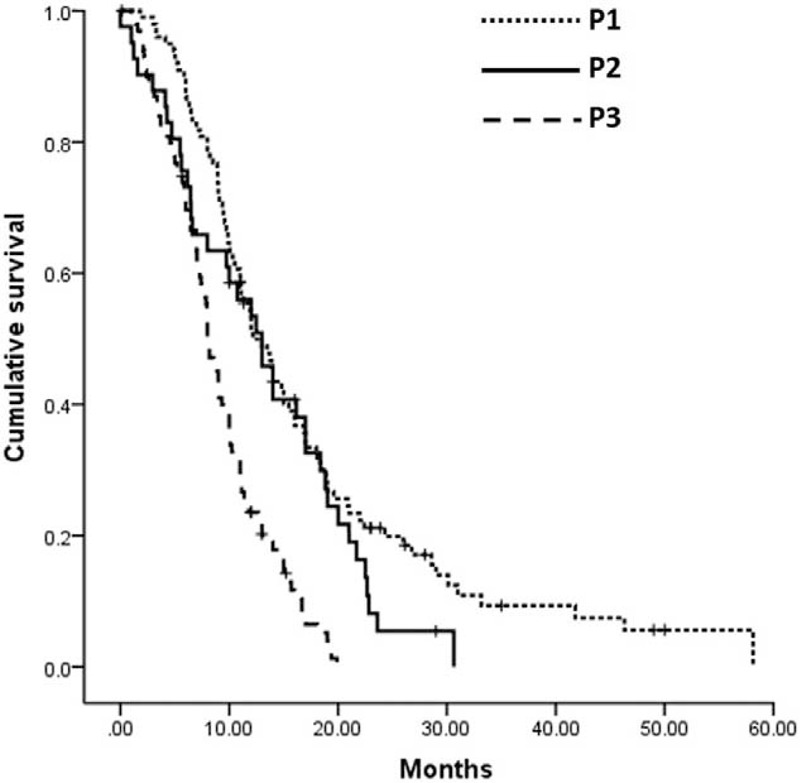
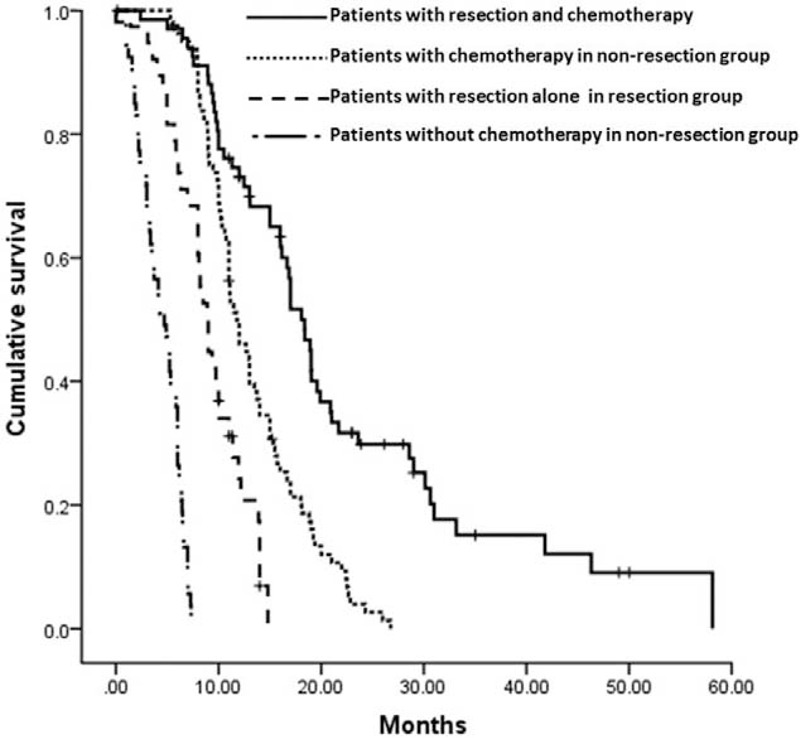
The aim of this study was to evaluate the survival benefit of palliative gastrectomy for gastric cancer patients with peritoneal seeding proven intraoperatively and to identify positive predictive factors for improving survival.The value of palliative resection for gastric cancer patients with peritoneal metastasis is controversial.From 2006 to 2013, 267 gastric cancer patients with intraoperatively identified peritoneal dissemination were retrospectively analyzed. Patients were divided into resection group and nonresection group according to whether a palliative gastrectomy was performed. Clinicopathologic variables and survival were compared. Subgroup analyses stratified by clinicopathologic factors and multivariable analysis for overall survival were also performed.There were 114 patients in the resection group and 153 in nonresection group. The morbidities in the resection and nonresection groups were 14.91% and 5.88%, respectively (P = 0.014). There, however, was no difference in mortality between the 2 groups. The median survival time of patients in the resection group was longer than in nonresection group (14.00 versus 8.57 months, P = 0.000). The median survivals among the patients with different classifications of peritoneal metastasis were statistically significant (P = 0.000). Patients undergoing resection followed by chemotherapy had a significantly longer median survival, compared with that of patients who had chemotherapy alone, those who had resection alone, or those who had not received chemotherapy or resection (P = 0.000). Results of subgroup analyses showed that except for P3 patients and patients with multisite distant metastases, overall survival was significantly better in patients with palliative gastrectomy, compared with the nonresection group. In multivariate analysis, P3 disease (P = 0.000), absence of resection (P = 0.000), and lack of chemotherapy (P = 0.000) were identified as independently associated with poor survival.Palliative gastrectomy might be beneficial to the survival of gastric cancer patients with intraoperatively proven P1/P2 alone, rather than P3. Postoperative palliative chemotherapy could improve survival regardless of operation and should be recommended.
Conflict of interest statement
The authors report they have no conflicts of interest to disclose
Figures
Similar articles
-
Significant Role of Palliative Gastrectomy in Selective Gastric Cancer Patients with Peritoneal Dissemination: A Propensity Score Matching Analysis.Ann Surg Oncol. 2016 Nov;23(12):3956-3963. doi: 10.1245/s10434-016-5223-2. Epub 2016 Jul 5. Ann Surg Oncol. 2016. PMID: 27380641
-
Addition of peritonectomy to gastrectomy can predict good prognosis of gastric adenocarcinoma patients with intraoperatively proven single P1/P2 carcinomatosis.Tumour Biol. 2017 Jun;39(6):1010428317697567. doi: 10.1177/1010428317697567. Tumour Biol. 2017. PMID: 28618957
-
Predictive factors improving survival after gastrectomy in gastric cancer patients with peritoneal carcinomatosis.World J Surg. 2010 Mar;34(3):555-62. doi: 10.1007/s00268-010-0396-5. World J Surg. 2010. PMID: 20082194
-
Clinical pathway for the management of resectable gastric cancer with peritoneal seeding: best palliation with a ray of hope for cure.Oncology. 2000 Feb;58(2):96-107. doi: 10.1159/000012086. Oncology. 2000. PMID: 10705236 Review.
-
[Clinical significance and practice points of conversion therapy for gastric cancer with peritoneal metastasis].Zhonghua Wei Chang Wai Ke Za Zhi. 2017 Oct 25;20(10):1094-1098. Zhonghua Wei Chang Wai Ke Za Zhi. 2017. PMID: 29130218 Review. Chinese.
Cited by
-
Palliative gastrectomy plus chemotherapy versus chemotherapy alone for incurable advanced gastric cancer: a meta-analysis.Cancer Manag Res. 2018 Oct 26;10:4759-4771. doi: 10.2147/CMAR.S179368. eCollection 2018. Cancer Manag Res. 2018. PMID: 30464590 Free PMC article.
-
Selective Gastric Cancer Patients with Peritoneal Seeding Benefit from Gastrectomy after Palliative Chemotherapy: A Propensity Score Matching Analysis.J Cancer. 2017 Jul 20;8(12):2231-2237. doi: 10.7150/jca.18932. eCollection 2017. J Cancer. 2017. PMID: 28819425 Free PMC article.
-
Treatment Modality Based Survival in Gastric Carcinoma Patients with Stand-Alone Peritoneal Metastasis: a Case-Control Study.J Gastric Cancer. 2021 Jun;21(2):122-131. doi: 10.5230/jgc.2021.21.e12. Epub 2021 May 20. J Gastric Cancer. 2021. PMID: 34234974 Free PMC article.
-
A Bottleneck in Understanding Metastatic Cancer Stem Cell of Peritoneal Seeding from Gastric Cancer: A Null Result in Brief.J Cancer. 2017 Sep 16;8(16):3274-3277. doi: 10.7150/jca.21669. eCollection 2017. J Cancer. 2017. PMID: 29158800 Free PMC article.
-
Peri-operative Outcomes and Survival Following Palliative Gastrectomy for Gastric Cancer: a Systematic Review and Meta-analysis.J Gastrointest Cancer. 2021 Mar;52(1):41-56. doi: 10.1007/s12029-020-00519-4. Epub 2020 Sep 22. J Gastrointest Cancer. 2021. PMID: 32959118 Free PMC article.
References
-
- Jemal A, Bray F, Center MM, et al. Global cancer statistics. CA Cancer J Clin 2011; 61:69–90. - PubMed
-
- Songun I, Putter H, Kranenbarg EM, et al. Surgical treatment of gastric cancer: 15-year follow-up results of the randomised nationwide Dutch D1D2 trial. Lancet Oncol 2010; 11:439–449. - PubMed
-
- Noh SH, Park SR, Yang HK, et al. CLASSIC trial investigators Adjuvant capecitabine plus oxaliplatin for gastric cancer after D2 gastrectomy (CLASSIC): 5-year follow-up of an open-label, randomised phase 3 trial. Lancet Oncol 2014; 15:1389–1396. - PubMed
-
- Bang YJ, Van Cutsem E, Feyereislova A, et al. ToGA Trial Investigators Trastuzumab in combination with chemotherapy versus chemotherapy alone for treatment of HER2-positive advanced gastric or gastro-oesophageal junction cancer (ToGA): a phase 3, open-label, randomised controlled trial. Lancet 2010; 376:687–697. - PubMed
-
- Chen S, Li YF, Feng XY, et al. Significance of palliative gastrectomy for late-stage gastric cancer patients. J Surg Oncol 2012; 106:862–871. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
