

Comparative Effectiveness and Safety of Monodrug Therapies for Lower Urinary Tract Symptoms Associated With Benign Prostatic Hyperplasia: A Network Meta-analysis
- PMID: 26166130
- PMCID: PMC4504542
- DOI: 10.1097/MD.0000000000000974
Comparative Effectiveness and Safety of Monodrug Therapies for Lower Urinary Tract Symptoms Associated With Benign Prostatic Hyperplasia: A Network Meta-analysis
Abstract
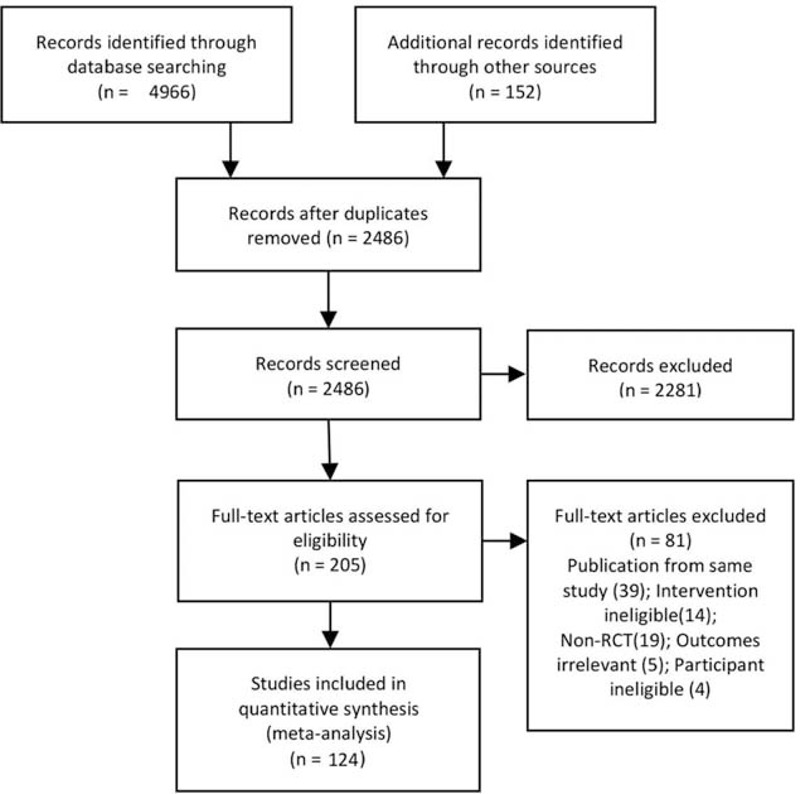
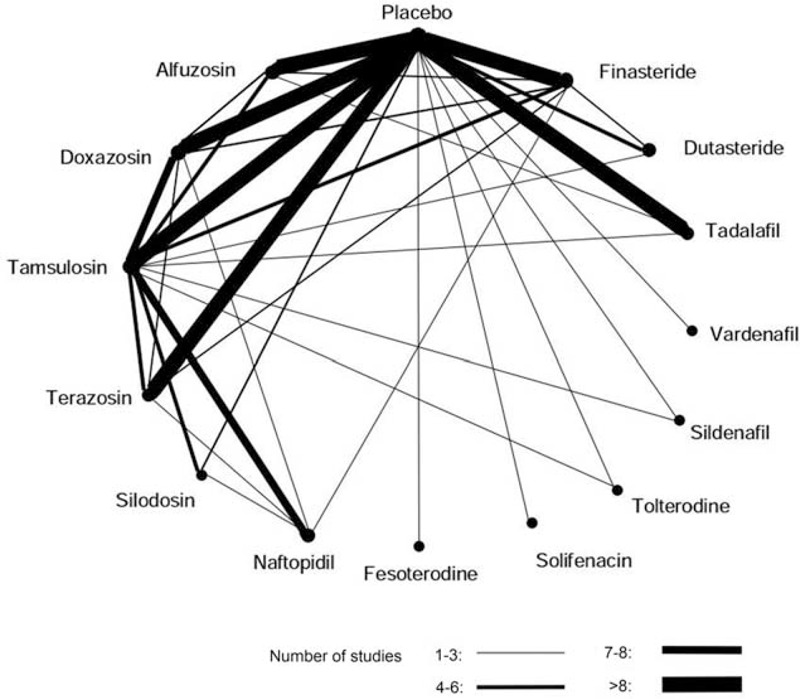
A wide array of drugs are available for the treatment of lower urinary tract symptoms associated with benign prostatic hyperplasia (BPH), but the evidence for the comparative effectiveness is controversial.The objective of this study is to evaluate the comparative effectiveness and safety of monodrug therapies for BPH.Data sources are MEDLINE, EMBASE, and the Cochrane Library.We included randomized controlled trials that compared α-blockers, 5-alpha reductase inhibitors (5ARIs), muscarinic receptor antagonists (MRAs), phosphodiesterase-5 inhibitor (PDE5-Is), or placebo for the treatment of BPH.Comparative effectiveness and safety were pooled by both traditional meta-analysis and network meta-analysis. Summary effect size was calculated as mean difference (MD) and relative risk (RR), together with the 95% confidence intervals (CIs).This study included 58,548 participants from 124 trials in total. When compared with placebo, α-blockers, 5ARIs, and PDE5-Is reduced International Prostate Symptom Score (IPSS) by -1.35 to -3.67 points and increased peak urinary flow rate (PUF) by -0.02 to 1.95 mL/s, with doxazosin (IPSS: MD, -3.67[-4.33 to -3.02]; PUF: MD, 1.95[1.61 to 2.30]) and terazosin (IPSS: MD, -3.37 [-4.24 to -2.50]; PUF: MD, 1.21[0.74 to 1.66]) showing the greatest improvement. The improvement in the IPSS was comparable among tamsulosin, alfuzosin, naftopidil, silodosin, dutasteride, sildenafil, vardenafil, and tadalafil. The incidence of total adverse events and withdraws due to adverse events were generally comparable among various agents.In conclusion, α-blockers, 5ARIs, and PDE5-Is are effective for BPH, with doxazosin and terazosin appearing to be the most effective agents. Drug therapies for BPH are generally safe and well-tolerated, with no major difference regarding the overall safety profile.
Conflict of interest statement
The authors have no funding and conflicts of interest to disclose.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
