

Awake craniotomy. A patient`s perspective
- PMID: 26166593
- PMCID: PMC4710339
- DOI: 10.17712/nsj.2015.3.20140548
Awake craniotomy. A patient`s perspective
Abstract
Objective: To report the personal experiences of patients undergoing awake craniotomy for brain tumor resection.
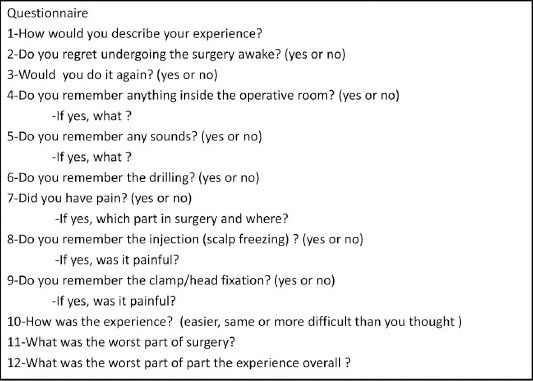
Methods: We carried out a qualitative descriptive survey of patients` experiences with awake craniotomies for brain tumor resection. The survey was conducted through a standard questionnaire form after the patient was discharged from the hospital.
Results: Of the 9 patients who met the inclusion criteria and underwent awake craniotomy, 3 of those patients reported no recollection of the operation. Five patients had auditory recollections from the operation. Two-thirds (6/9) reported that they did not perceive pain. Five patients remembered the head clamp fixation, and 2 of those patients classified the pain from the clamp as moderate. None of the patients reported that the surgery was more difficult than anticipated.
Conclusion: Awake craniotomy for surgical resection of brain tumors was well tolerated by patients. Most patients reported that they do not recall feeling pain during the operation. However, we feel that further work and exploration are needed in order to achieve better control of pain and discomfort during these types of operations.
Figures


Similar articles
-
Patients' perspective on awake craniotomy for brain tumors-single center experience in Brazil.Acta Neurochir (Wien). 2017 Apr;159(4):725-731. doi: 10.1007/s00701-017-3125-0. Epub 2017 Feb 28. Acta Neurochir (Wien). 2017. PMID: 28247161
-
Compassion, communication, and the perception of control: a mixed methods study to investigate patients' perspectives on clinical practices for alleviating distress and promoting empowerment during awake craniotomies.Br J Neurosurg. 2024 Aug;38(4):911-922. doi: 10.1080/02688697.2021.2005773. Epub 2021 Dec 1. Br J Neurosurg. 2024. PMID: 34850642 Free PMC article.
-
Patient acceptance of awake craniotomy.Clin Neurol Neurosurg. 2011 Dec;113(10):880-4. doi: 10.1016/j.clineuro.2011.06.010. Epub 2011 Jul 23. Clin Neurol Neurosurg. 2011. PMID: 21782320
-
Patient response to awake craniotomy - a summary overview.Acta Neurochir (Wien). 2014 Jun;156(6):1063-70. doi: 10.1007/s00701-014-2038-4. Epub 2014 Mar 5. Acta Neurochir (Wien). 2014. PMID: 24595540 Review.
-
Patient-reported intraoperative experiences during awake craniotomy for brain tumors: a scoping review.Neurosurg Rev. 2022 Oct;45(5):3093-3107. doi: 10.1007/s10143-022-01833-0. Epub 2022 Jul 11. Neurosurg Rev. 2022. PMID: 35816270
Cited by
-
Permutation entropy in intraoperative ECoG of brain tumour patients in awake tumour surgery- a robust parameter to separate consciousness from unconsciousness.Sci Rep. 2019 Nov 11;9(1):16482. doi: 10.1038/s41598-019-52949-1. Sci Rep. 2019. PMID: 31712616 Free PMC article.
-
Surgical Treatment of Glioblastoma: State-of-the-Art and Future Trends.J Clin Med. 2022 Sep 13;11(18):5354. doi: 10.3390/jcm11185354. J Clin Med. 2022. PMID: 36143001 Free PMC article. Review.
-
The Awake Craniotomy: A Patient's Experience and A Literature Review.Cureus. 2022 Jun 29;14(6):e26441. doi: 10.7759/cureus.26441. eCollection 2022 Jun. Cureus. 2022. PMID: 35915692 Free PMC article.
-
What is the advance of extent of resection in glioblastoma surgical treatment-a systematic review.Chin Neurosurg J. 2019 Feb 1;5:2. doi: 10.1186/s41016-018-0150-7. eCollection 2019. Chin Neurosurg J. 2019. PMID: 32922902 Free PMC article. Review.
-
Advances in Brain Tumor Surgery for Glioblastoma in Adults.Brain Sci. 2017 Dec 20;7(12):166. doi: 10.3390/brainsci7120166. Brain Sci. 2017. PMID: 29261148 Free PMC article. Review.
References
-
- Penfield W, Pasquet A. Combined regional and general anesthesia for craniotomy and cortical exploration. Part I. Neurosurgical considerations. Int Anesthesiol Clin. 1986;24:1–20. - PubMed
-
- Bulsara KR, Johnson J, Villavicencio AT. Improvements in brain tumor surgery: the modern history of awake craniotomies. Neurosurg Focus. 2005;18:e5. - PubMed
-
- Costello TG, Cormack JR. Anaesthesia for awake craniotomy: a modern approach. J Clin Neurosci. 2004;11:16–19. - PubMed
-
- Meyer FB, Bates LM, Goerss SJ, Friedman JA, Windschitl WL, Duffy JR, et al. Awake craniotomy for aggressive resection of primary gliomas located in eloquent brain. Mayo Clin Proc. 2001;76:677–687. - PubMed
-
- Blanshard HJ, Chung F, Manninen PH, Taylor MD, Bernstein M. Awake craniotomy for removal of intracranial tumor: considerations for early discharge. Anesth Analg. 2001;92:89–94. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous