

Targeted Prostate Biopsy: Lessons Learned Midst the Evolution of a Disruptive Technology
- PMID: 26166671
- PMCID: PMC4569505
- DOI: 10.1016/j.urology.2015.07.001
Targeted Prostate Biopsy: Lessons Learned Midst the Evolution of a Disruptive Technology
Abstract
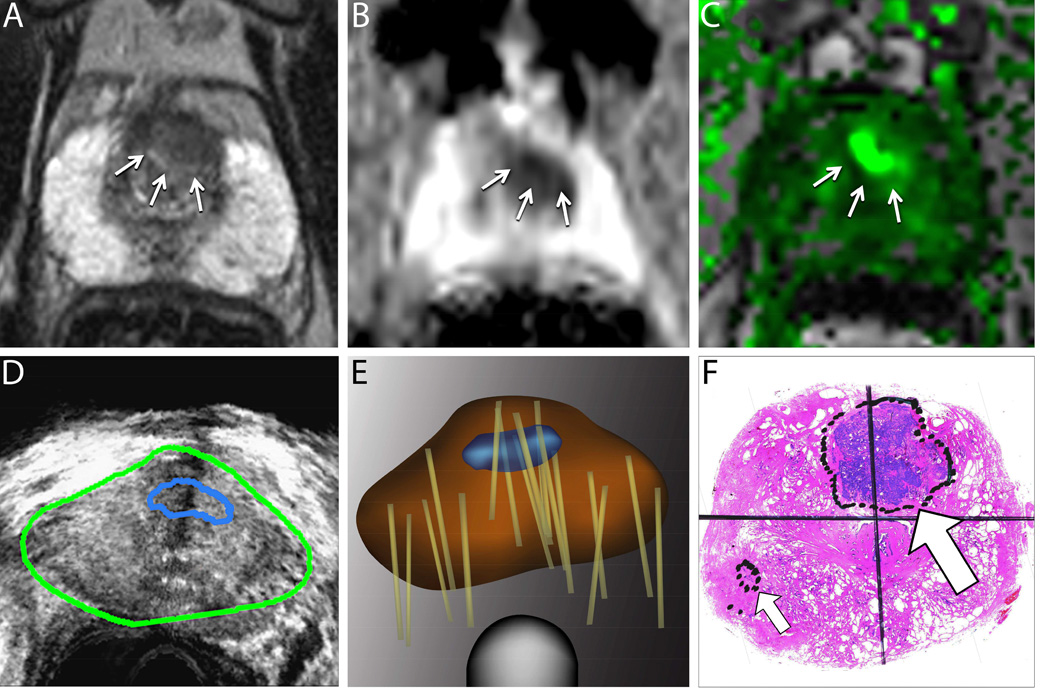
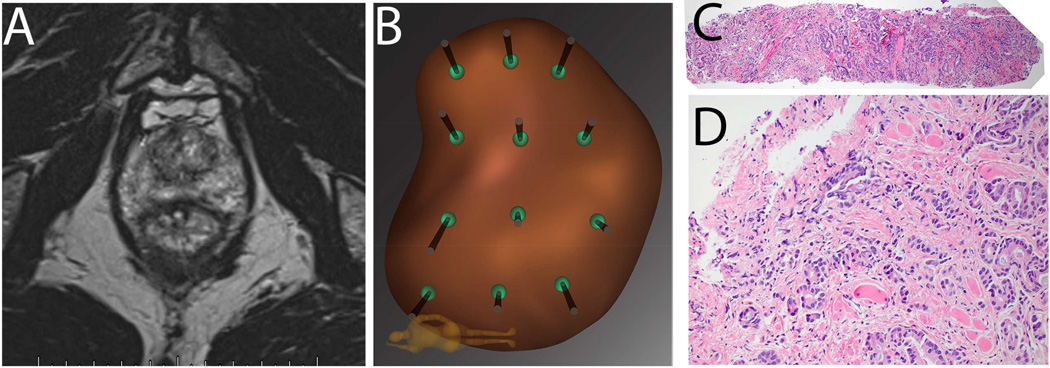
Lessons learned during a 6-year experience with more than 1200 patients undergoing targeted prostate biopsy via MRI/ultrasound fusion are reported: (1) the procedure is safe and efficient, requiring some 15-20 minutes in an office setting; (2) MRI is best performed by a radiologist with specialized training, using a transabdominal multiparametric approach and preferably a 3T magnet; (3) grade of MRI suspicion is the most powerful predictor of biopsy results, eg, Grade 5 usually represents cancer; (4) some potentially important cancers (15%-30%) are MRI-invisible; (5) Targeted biopsies provide >80% concordance with whole-organ pathology. Early enthusiasm notwithstanding, cost-effectiveness is yet to be resolved, and the technologies remain in evolution.
Copyright © 2015 Elsevier Inc. All rights reserved.
Figures
Similar articles
-
In-Bore MR-Guided Biopsy Systems and Utility of PI-RADS.Top Magn Reson Imaging. 2016 Jun;25(3):119-23. doi: 10.1097/RMR.0000000000000090. Top Magn Reson Imaging. 2016. PMID: 27187168
-
A role of multifactorial evaluation of prostatic 3T MRI in patients with elevated prostatic-specific antigen levels: prospective comparison with ultrasound-guided transrectal biopsy.Anticancer Res. 2013 Jun;33(6):2791-5. Anticancer Res. 2013. PMID: 23749943
-
Targeted MRI-guided prostate biopsies for the detection of prostate cancer: initial clinical experience with real-time 3-dimensional transrectal ultrasound guidance and magnetic resonance/transrectal ultrasound image fusion.Urology. 2013 Jun;81(6):1372-8. doi: 10.1016/j.urology.2013.02.022. Epub 2013 Mar 26. Urology. 2013. PMID: 23540865 Clinical Trial.
-
Multiparametric magnetic resonance imaging in the detection of prostate cancer.Aktuelle Urol. 2014 Mar;45(2):119-26. doi: 10.1055/s-0034-1371875. Epub 2014 Apr 3. Aktuelle Urol. 2014. PMID: 24700068 Review.
-
Multiparametric magnetic resonance imaging in the detection of prostate cancer.Rofo. 2014 Mar;186(3):238-46. doi: 10.1055/s-0034-1365937. Epub 2014 Jan 22. Rofo. 2014. PMID: 24452493 Review.
Cited by
-
Transperineal prostate biopsy identifies locations of clinically significant prostate cancer in men considering focal therapy with PI-RADS 3-5 regions of interest.BJUI Compass. 2021 Oct 5;2(6):395-401. doi: 10.1002/bco2.111. eCollection 2021 Nov. BJUI Compass. 2021. PMID: 35474703 Free PMC article.
-
Identifying Risk Factors for MRI-Invisible Prostate Cancer in Patients Undergoing Transperineal Saturation Biopsy.Res Rep Urol. 2021 Sep 27;13:723-731. doi: 10.2147/RRU.S323823. eCollection 2021. Res Rep Urol. 2021. PMID: 34611522 Free PMC article.
-
Reproducibility of Multiparametric Magnetic Resonance Imaging and Fusion Guided Prostate Biopsy: Multi-Institutional External Validation by a Propensity Score Matched Cohort.J Urol. 2016 Jun;195(6):1737-43. doi: 10.1016/j.juro.2015.12.102. Epub 2016 Jan 23. J Urol. 2016. PMID: 26812301 Free PMC article. Clinical Trial.
-
Evaluation of Matrix Metalloproteases by Artificial Intelligence Techniques in Negative Biopsies as New Diagnostic Strategy in Prostate Cancer.Int J Mol Sci. 2023 Apr 10;24(8):7022. doi: 10.3390/ijms24087022. Int J Mol Sci. 2023. PMID: 37108185 Free PMC article.
-
Magnetic resonance imaging for prostate cancer before radical and salvage radiotherapy: What radiation oncologists need to know.World J Clin Oncol. 2017 Aug 10;8(4):305-319. doi: 10.5306/wjco.v8.i4.305. World J Clin Oncol. 2017. PMID: 28848697 Free PMC article. Review.
References
-
- Bower JL, Christensen CM. Disruptive Technologies - Catching the Wave. Harvard Bus Rev. 1995;73:43–53. PMID:ISI:A1995PZ57400009.
-
- Hodge KK, McNeal JE, Terris MK, Stamey TA. Random systematic versus directed ultrasound guided transrectal core biopsies of the prostate. The Journal of urology. 1989;142:71–74. discussion 4–5 PMID:2659827. - PubMed
-
- Welch HG, Fisher ES, Gottlieb DJ, Barry MJ. Detection of prostate cancer via biopsy in the Medicare-SEER population during the PSA era. Journal of the National Cancer Institute. 2007;99:1395–1400. PMID:17848671. - PubMed
-
- Autorino R, De Sio M, Di Lorenzo G, et al. How to decrease pain during transrectal ultrasound guided prostate biopsy: a look at the literature. The Journal of urology. 2005;174:2091–2097. PMID:16280735. - PubMed
-
- Eichler K, Hempel S, Wilby J, Myers L, Bachmann LM, Kleijnen J. Diagnostic value of systematic biopsy methods in the investigation of prostate cancer: a systematic review. The Journal of urology. 2006;175:1605–1612. PMID:16600713. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
