

Rectal cancer: An evidence-based update for primary care providers
- PMID: 26167068
- PMCID: PMC4491955
- DOI: 10.3748/wjg.v21.i25.7659
Rectal cancer: An evidence-based update for primary care providers
Abstract
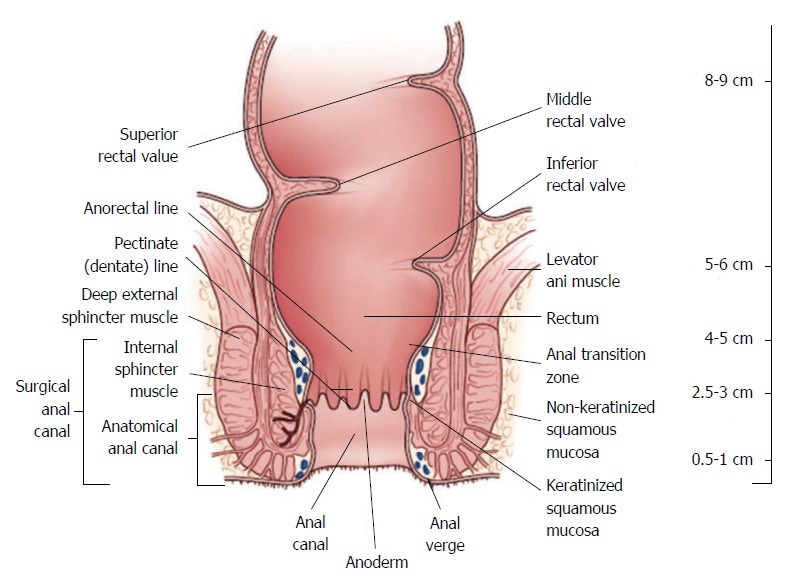
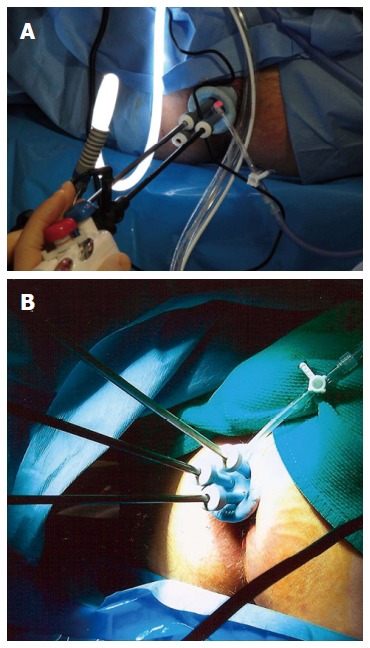
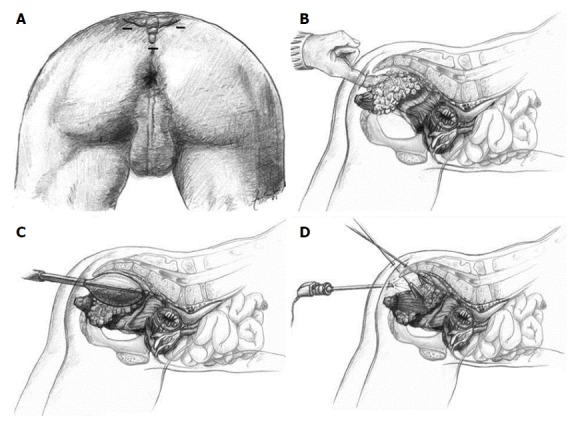
Rectal adenocarcinoma is an important cause of cancer-related deaths worldwide, and key anatomic differences between the rectum and the colon have significant implications for management of rectal cancer. Many advances have been made in the diagnosis and management of rectal cancer. These include clinical staging with imaging studies such as endorectal ultrasound and pelvic magnetic resonance imaging, operative approaches such as transanal endoscopic microsurgery and laparoscopic and robotic assisted proctectomy, as well as refined neoadjuvant and adjuvant therapies. For stage II and III rectal cancers, combined chemoradiotherapy offers the lowest rates of local and distant relapse, and is delivered neoadjuvantly to improve tolerability and optimize surgical outcomes, particularly when sphincter-sparing surgery is an endpoint. The goal in rectal cancer treatment is to optimize disease-free and overall survival while minimizing the risk of local recurrence and toxicity from both radiation and systemic therapy. Optimal patient outcomes depend on multidisciplinary involvement for tailored therapy. The successful management of rectal cancer requires a multidisciplinary approach, with the involvement of enterostomal nurses, gastroenterologists, medical and radiation oncologists, radiologists, pathologists and surgeons. The identification of patients who are candidates for combined modality treatment is particularly useful to optimize outcomes. This article provides an overview of the diagnosis, staging and multimodal therapy of patients with rectal cancer for primary care providers.
Keywords: Diagnosis; Primary care; Rectal cancer; Review; Treatment.
Figures
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2015. CA Cancer J Clin. 2015;65:5–29. - PubMed
-
- Nelson H, Petrelli N, Carlin A, Couture J, Fleshman J, Guillem J, Miedema B, Ota D, Sargent D. Guidelines 2000 for colon and rectal cancer surgery. J Natl Cancer Inst. 2001;93:583–596. - PubMed
-
- Apgar BS, Brotzman GL, Spitzer M, editors . Colposcopy principles and practice, 2nd ed. Saunders: Philadelphia; 2008.
-
- Glynne-Jones R, Mathur P, Elton C, Train ML. The multidisciplinary management of gastrointestinal cancer. Multimodal treatment of rectal cancer. Best Pract Res Clin Gastroenterol. 2007;21:1049–1070. - PubMed
-
- Heald RJ, Ryall RD. Recurrence and survival after total mesorectal excision for rectal cancer. Lancet. 1986;1:1479–1482. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
