

T lymphocytes and fractalkine contribute to myocardial ischemia/reperfusion injury in patients
- PMID: 26168217
- PMCID: PMC4563749
- DOI: 10.1172/JCI80055
T lymphocytes and fractalkine contribute to myocardial ischemia/reperfusion injury in patients
Abstract
Background: Lymphocytes contribute to ischemia/reperfusion (I/R) injury in several organ systems, but their relevance in ST elevation myocardial infarction (STEMI) is unknown. Our goal was to characterize lymphocyte dynamics in individuals after primary percutaneous coronary intervention (PPCI), assess the prognostic relevance of these cells, and explore mechanisms of lymphocyte-associated injury.
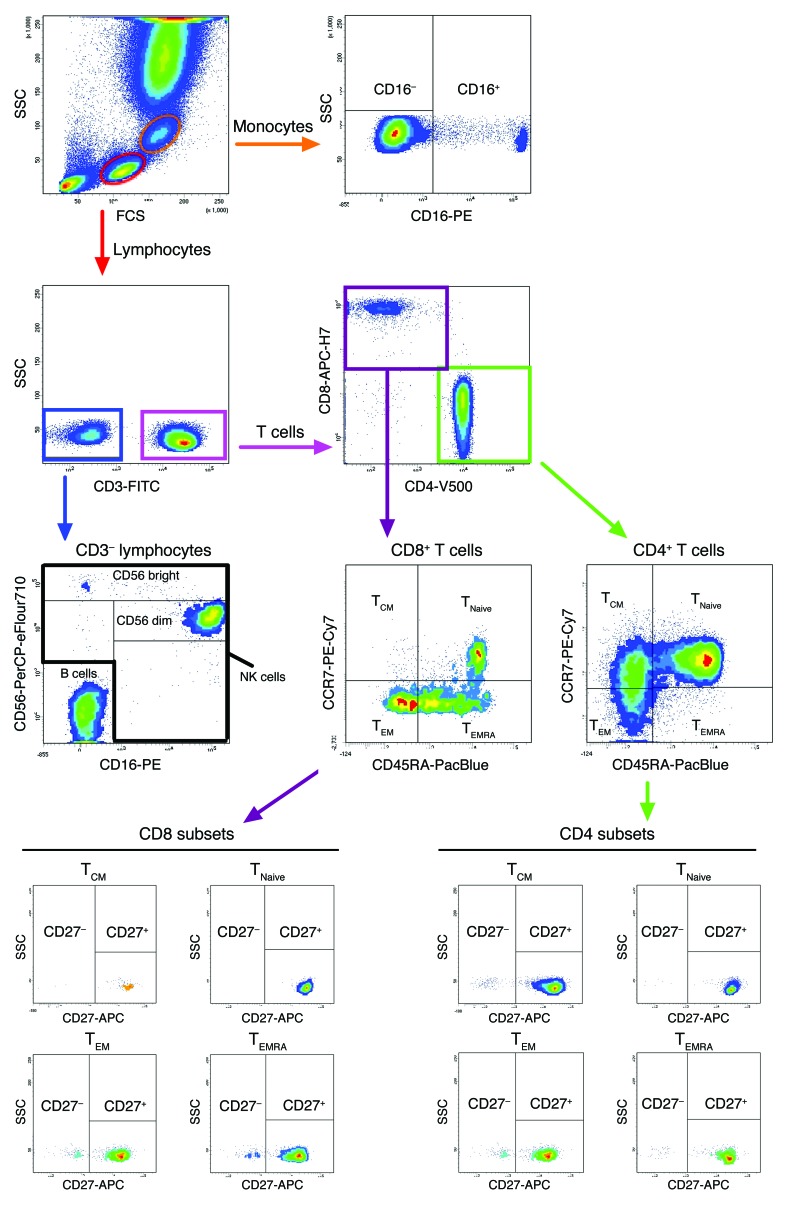
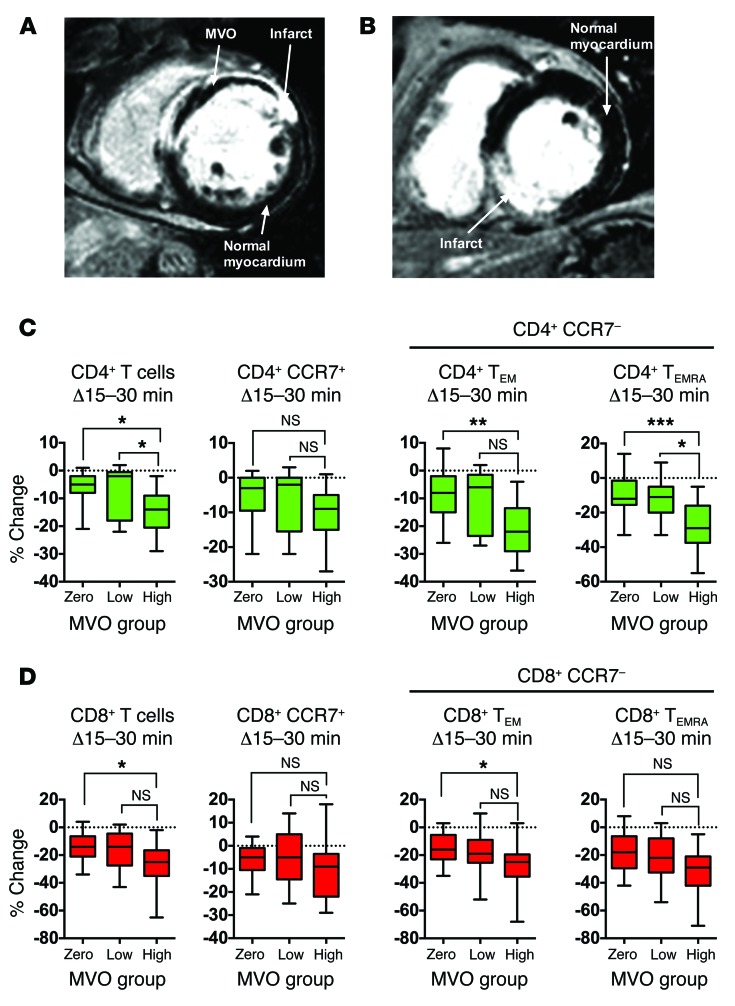
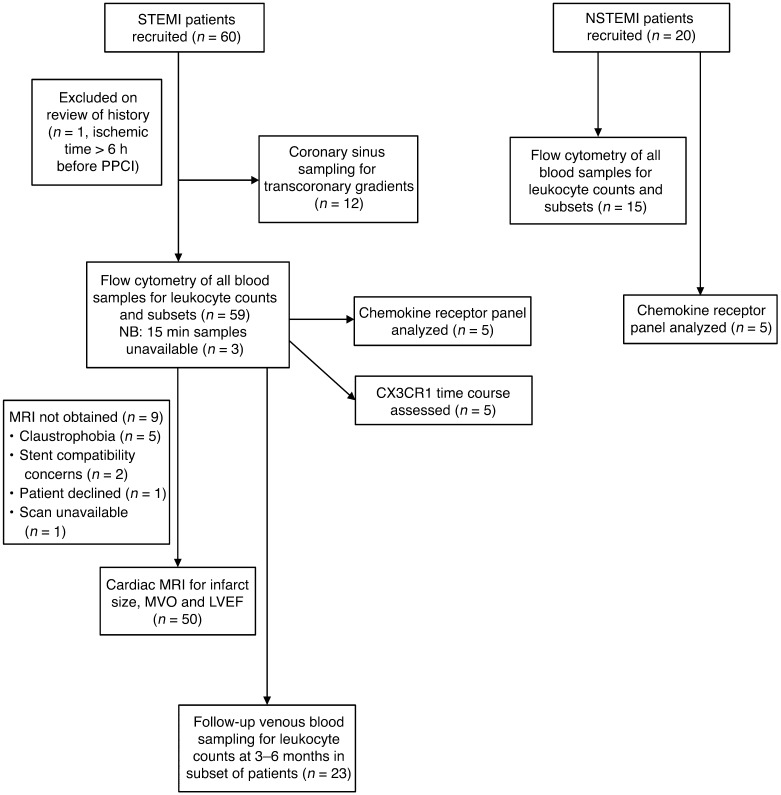
Methods: Lymphocyte counts were retrospectively analyzed in 1,377 STEMI patients, and the prognostic relevance of post-PPCI lymphopenia was assessed by Cox proportional hazards regression. Blood from 59 prospectively recruited STEMI patients undergoing PPCI was sampled, and leukocyte subpopulations were quantified. Microvascular obstruction (MVO), a component of I/R injury, was assessed using MRI.
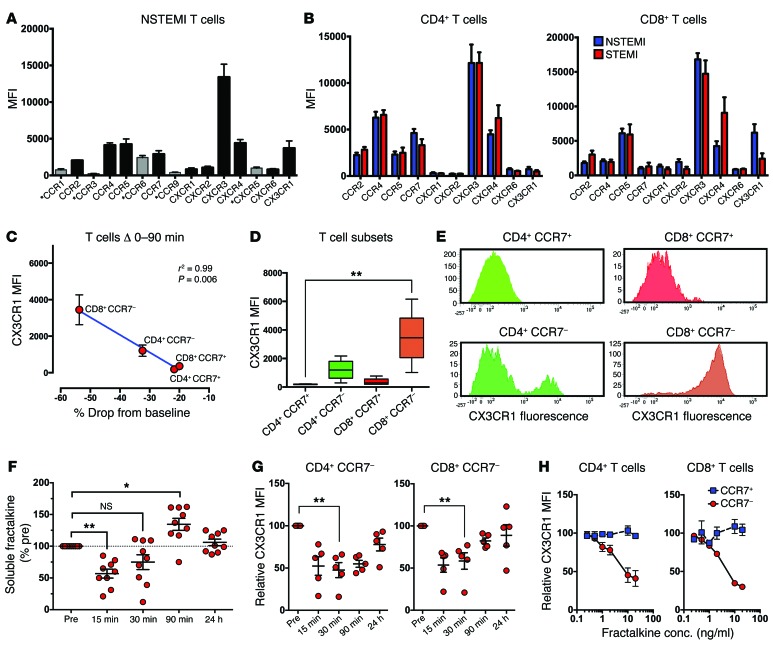
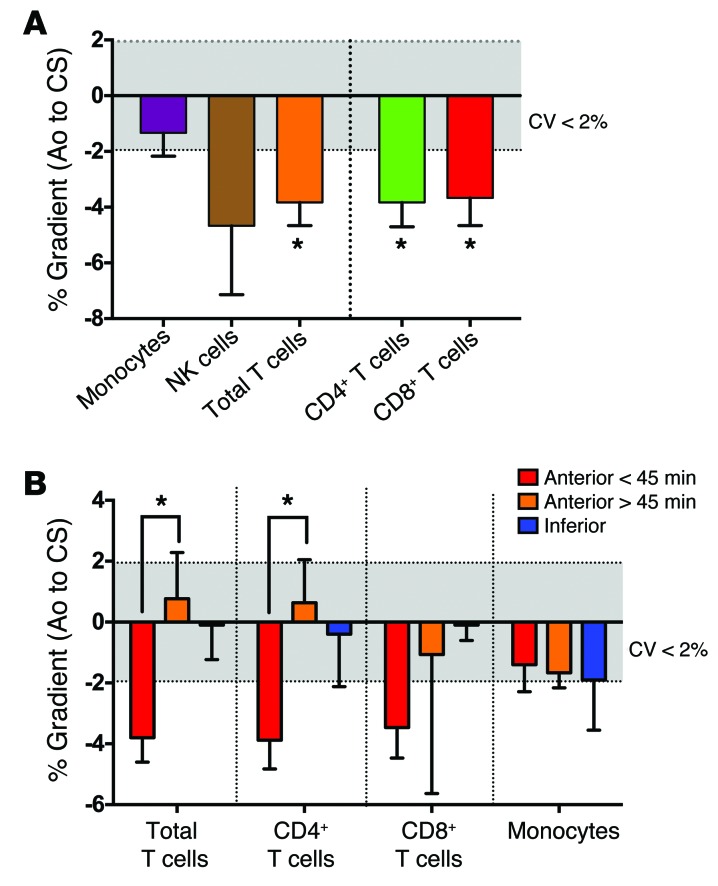
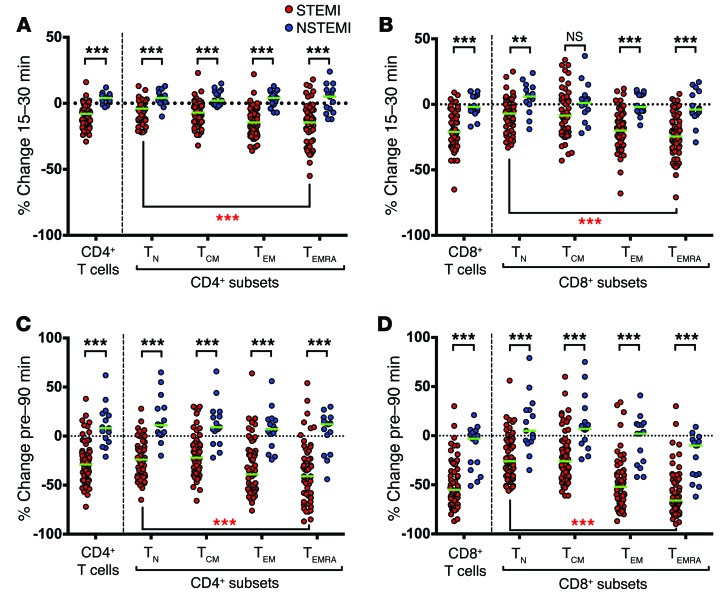
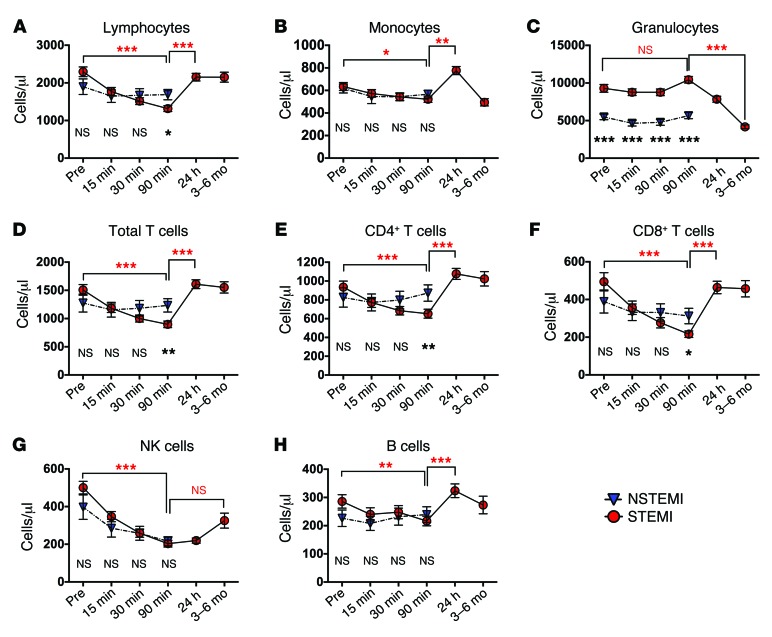
Results: In the retrospective cohort, lymphopenia was associated with a lower rate of survival at 3 years (82.8% vs. 96.3%, lowest vs. highest tertile; hazard ratio 2.42). In the prospective cohort, lymphocyte counts fell 90 minutes after reperfusion, primarily due to loss of T cells. CD8+ T cells decreased more than CD4+ T cells, and effector subsets exhibited the largest decline. The early decrease in effector T cell levels was greater in individuals that developed substantial MVO. The drop in T cell subsets correlated with expression of the fractalkine receptor CX3CR1 (r2 = 0.99, P = 0.006). Serum fractalkine concentration peaked at 90 minutes after reperfusion, coinciding with the T cell count nadir.
Conclusions: Lymphopenia following PPCI is associated with poor prognosis. Our data suggest that fractalkine contributes to lymphocyte shifts, which may influence development of MVO through the action of effector T cells.
Trial registration: Not applicable.
Funding: British Heart Foundation (FS/12/31/29533) and National Institute of Health Research (NIHR) Newcastle Biomedical Research Centre.
Figures

References
-
- Ito H. No-reflow phenomenon in patients with acute myocardial infarction: its pathophysiology and clinical implications. Acta Med Okayama. 2009;63(4):161–168. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
