

The Norwood operation: Relative effects of surgeon and institutional volumes on outcomes and resource utilization
- PMID: 26169083
- PMCID: PMC4713384
- DOI: 10.1017/S1047951115001031
The Norwood operation: Relative effects of surgeon and institutional volumes on outcomes and resource utilization
Abstract
Background: Hypoplastic left heart syndrome is the most expensive birth defect managed in the United States, with a 5-year survival rate below 70%. Increasing evidence suggests that hospital volumes are inversely associated with mortality for infants with single ventricles undergoing stage 1 surgical palliation. Our aim was to examine the relative effects of surgeon and institutional volumes on outcomes and resource utilisation for these children.
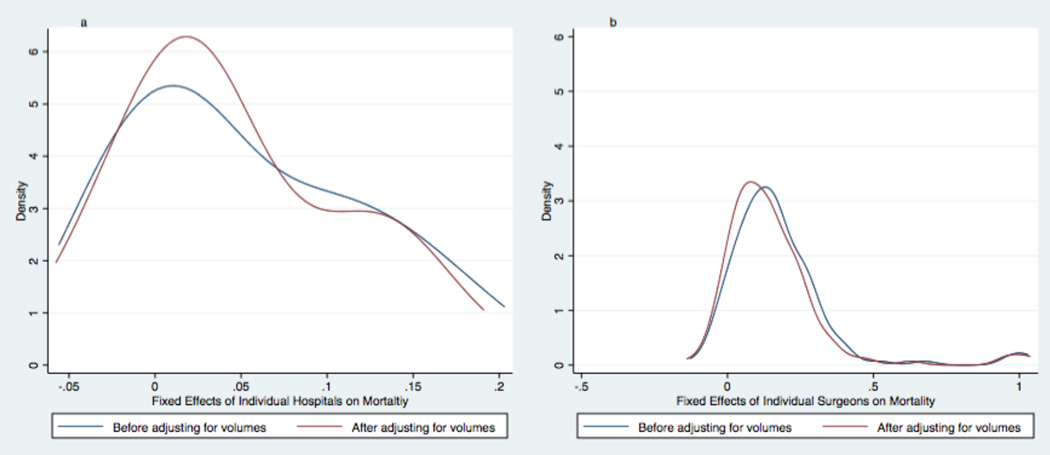
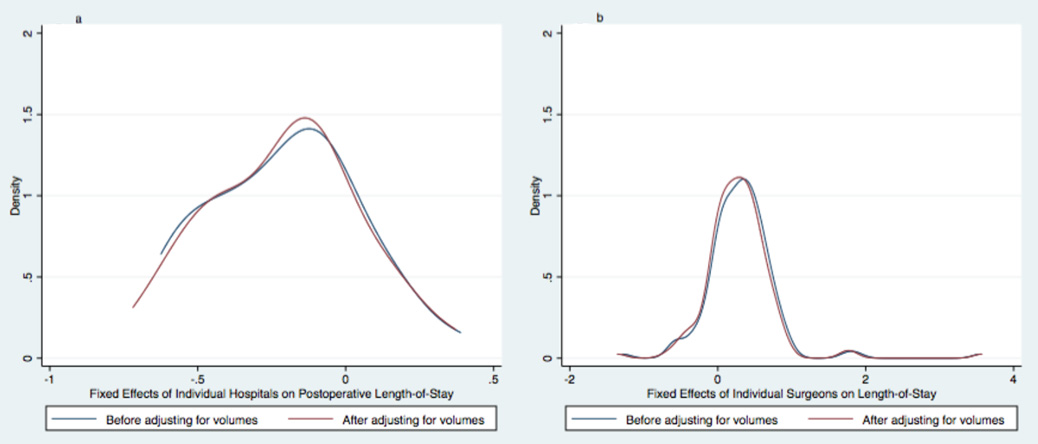
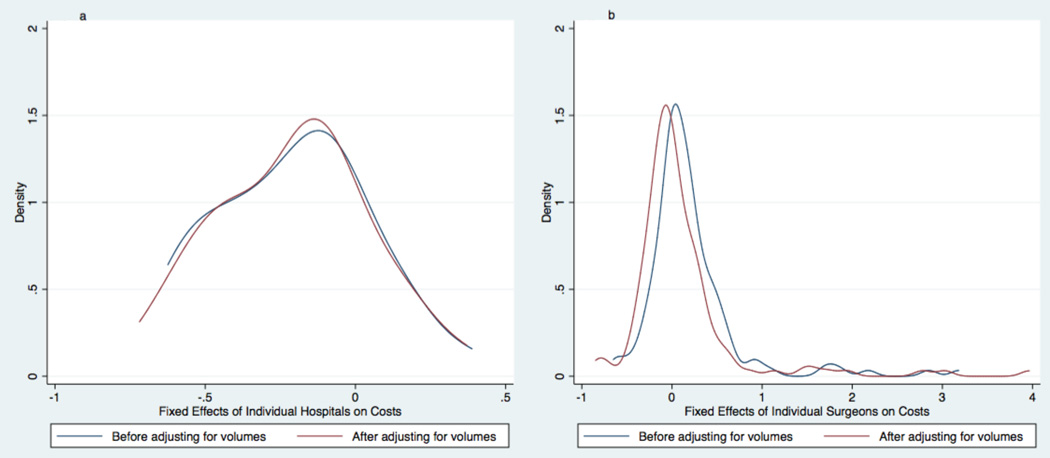
Methods: A retrospective study was conducted using the Pediatric Health Information System database to examine the effects of the number of procedures performed per surgeon and per centre on mortality, costs, and post-operative length of stay for infants undergoing Risk Adjustment for Congenital Heart Surgery risk category six operations at tertiary-care paediatric hospitals, from 1 January, 2004 to 31 December, 2013. Multivariable modelling was used, adjusting for patient and institutional characteristics. Gaussian kernel densities were constructed to show the relative distributions of the effects of individual institutions and surgeons, before and after adjusting for the number of cases performed.
Results: A total of 2880 infants from 35 institutions met the inclusion criteria. Mortality was 15.0%. Median post-operative length of stay was 24 days (IQR 14-41). Median standardized inpatient hospital costs were $156,000 (IQR $108,000-$248,000) in 2013 dollars. In the multivariable analyses, higher institutional volume was inversely associated with mortality (p=0.001), post-operative length of stay (p=0.004), and costs (p=0.001). Surgeon volume was associated with none of the measured outcomes. Neither institutional nor surgeon volumes explained much of the wide variation in outcomes and resource utilization observed between institutions and between surgeons.
Conclusions: Increased institutional - but not surgeon - volumes are associated with reduced mortality, post-operative length of stay, and costs for infants undergoing stage 1 palliation.
Keywords: Hypoplastic left heart syndrome; Norwood; costs; outcomes; surgeon volume.
Conflict of interest statement
None
Figures
References
-
- Robbins JM, Bird TM, Tilford JM, et al. Hospital Stays, Hospital Charges, and In-Hospital Deaths Among Infants with Selected Birth Defects--United States, 2003. Morbidity and Mortality Weekly Report. 2007;56:25–29. - PubMed
-
- Bazzani LG, Marcin JP. Case volume and mortality in pediatric cardiac surgery patients in California, 1998–2003. Circulation. 2007;115:2652–2659. - PubMed
-
- Jenkins KJ, Newburger JW, Lock JE, et al. In-hospital mortality for surgical repair of congenital heart defects: preliminary observations of variation by hospital caseload. Pediatrics. 1995;95:323–330. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
