

The use of telemedicine in burn care: development of a mobile system for TBSA documentation and remote assessment
- PMID: 26170783
- PMCID: PMC4396802
The use of telemedicine in burn care: development of a mobile system for TBSA documentation and remote assessment
Abstract
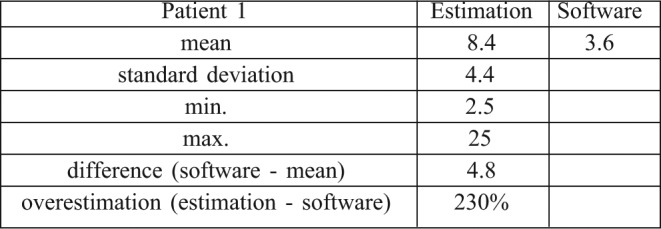
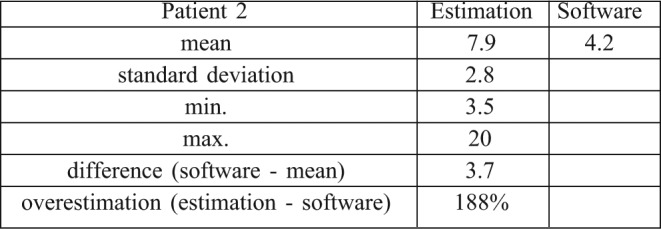
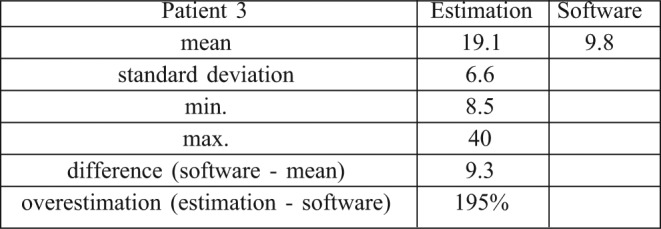
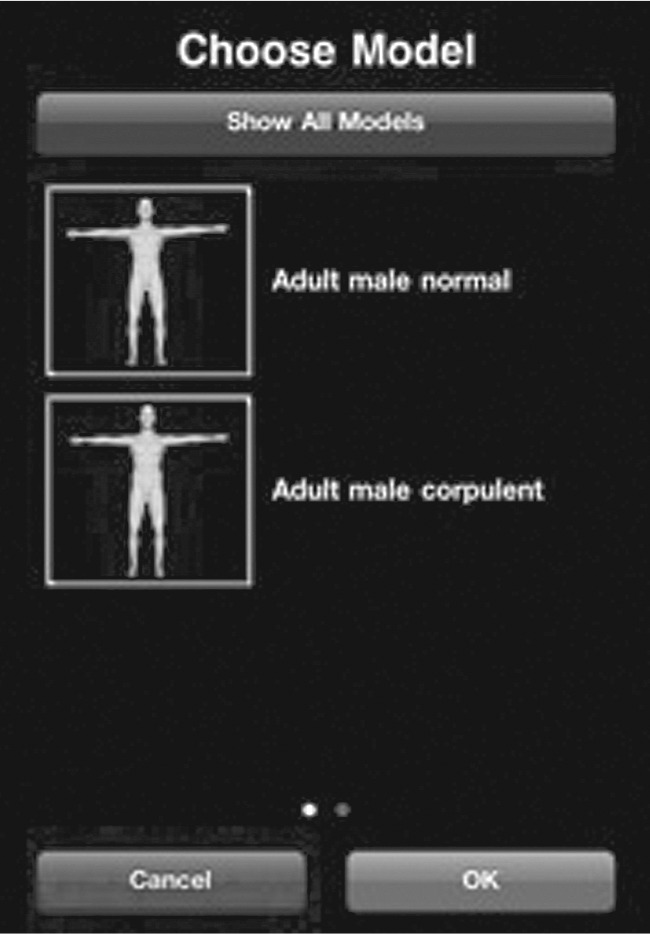
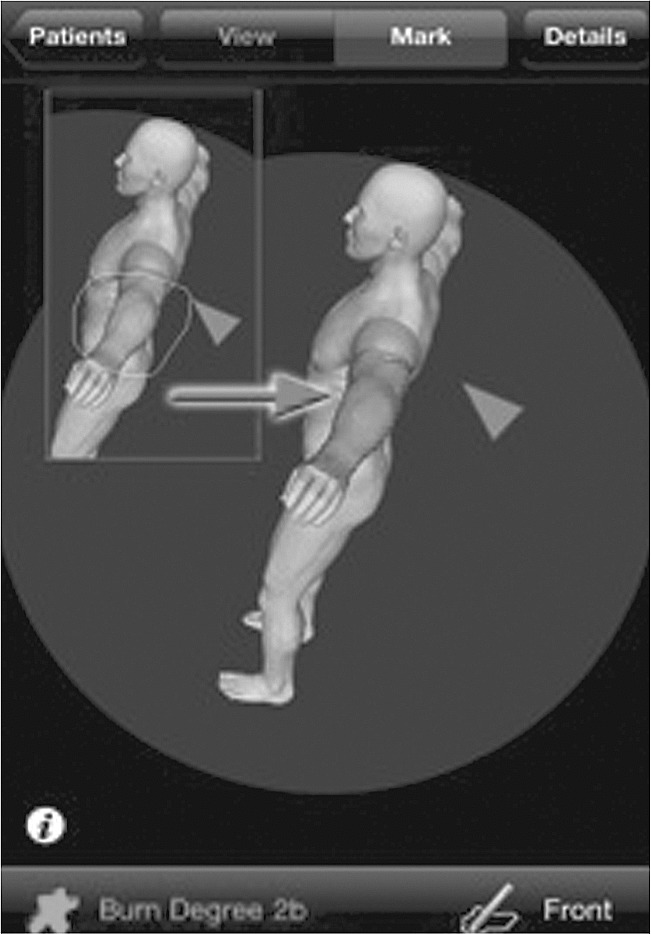
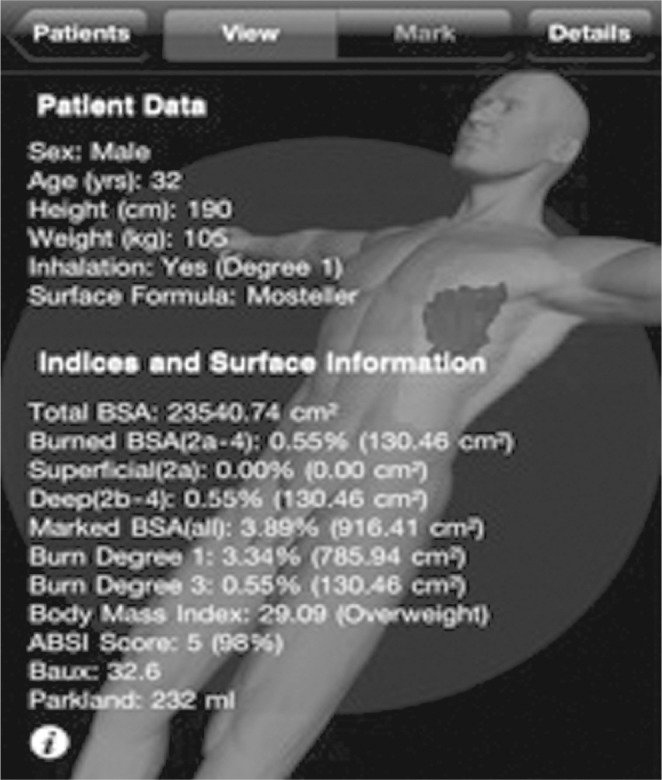
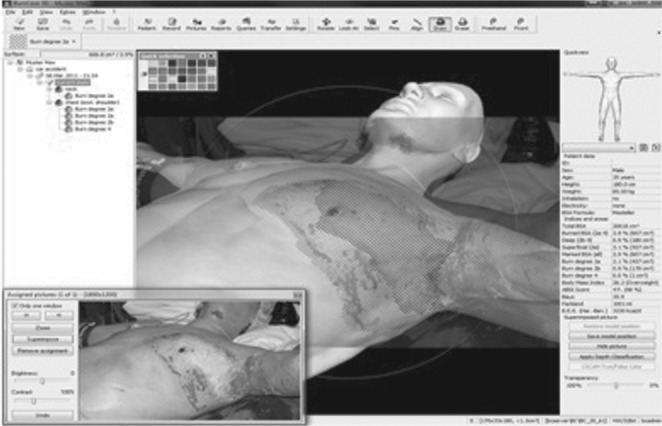
The requirements for accurate documentation within the process of burn assessment have increased dramatically over the years. TBSA (total body surface area) and burn depth are commonly determined by visual inspection, especially in the emergency or acute care setting. However, inexperience often results in incorrect estimation of these factors. In 2001, BurnCase 3D was initiated in order to develop a tool for objective burn assessment and documentation on mobile devices (Apple iPhoneTM). The centerpiece is a 3D model representing the actual patient. At two international burn meetings, a survey containing three pictures of patients was conducted and this data was collected. A patient-specific 3D model adapted to the height and weight of the real patient was created and the digital picture was superimposed in the computer system. The burns were transferred to the model and the TBSA in % was calculated by the software BurnCase 3D. The preferred methods of the 80 respondents for burn extent estimation were: the Rule of Nines (38%), the Rule of Palm (37%) and the Lund-Browder chart (18%). Analysis showed very high deviations of TBSA within the participants, even among the group of experts. In comparison to a computer-aided method we found massive overestimation of up to 230%. The use of BurnCase 3D could have a true impact on the quality of treatment in burns. In the acute care setting for burn injuries, telemedicine has great potential to help guide decisions regarding triage and transfer based on TBSA, burn depth, patient age and injury mechanism.
Les exigences en matière de documentation précise dans le processus de l’évaluation des brûlures ont augmenté de façon spectaculaire au cours des années. La SCT (surface corporelle totale) et la profondeur de la brûlure sont généralement déterminées par inspection visuelle, en particulier dans le contexte d’urgence ou de soins aigus. Cependant, l’inexpérience se traduit souvent par une estimation incorrecte de ces facteurs. En 2001, BurnCase 3D a été lancé afin de développer un outil d’évaluation des brûlures objectif et de la documentation sur les appareils mobiles d’Apple (iPhone™). La pièce maîtresse est un modèle 3D représentant le patient réel. Sur deux réunions de brûlures internationales, une enquête contenant trois photos de patients a été réalisée. Ces données ont été collectées. Un modèle 3D spécifique au patient adapté à la taille et le poids du patient réel a été créé et l’image a été superposée dans le système informatique. Les brûlures ont été transférés dans le modèle et le % de la surface corporelle totale a été calculé par le logiciel BurnCase 3D. Les méthodes préférées des 80 répondants pour l’estimation de la taille de la brûlure étaient : la règle des neuf (38%), la règle des palm (37%) et les tables de Lund et Browder (18%). L’analyse montre des écarts très élevés de SCT dans les participants, même parmi le groupe d’experts. Par rapport à un procédé assisté par ordinateur, nous avons trouvé surestimation massive de jusqu’à 230%. L’utilisation de BurnCase 3D pourrait avoir un véritable impact sur la qualité du traitement des brûlures. Dans le cadre de soins de courte durée pour les brûlures, la télémédecine a un grand potentiel pour aider à guider les décisions concernant le triage et le transfert sur la base de la SCT et la profondeur de la brûlure, l’âge du patient et le mécanisme de blessure.
Keywords: BurnCase 3D; TBSA; application; burn injuries; telemedicine.
Figures



Similar articles
-
Practical Computer Vision Application to Compute Total Body Surface Area Burn: Reappraising a Fundamental Burn Injury Formula in the Modern Era.JAMA Surg. 2022 Feb 1;157(2):129-135. doi: 10.1001/jamasurg.2021.5848. JAMA Surg. 2022. PMID: 34817552 Free PMC article.
-
Comparison of two-dimensional methods versus three-dimensional scanning systems in the assessment of total body surface area estimation in burn patients.Burns. 2018 Feb;44(1):195-200. doi: 10.1016/j.burns.2017.07.003. Epub 2017 Aug 7. Burns. 2018. PMID: 28797577
-
Technical and Medical Aspects of Burn Size Assessment and Documentation.Medicina (Kaunas). 2021 Mar 5;57(3):242. doi: 10.3390/medicina57030242. Medicina (Kaunas). 2021. PMID: 33807630 Free PMC article. Review.
-
Accuracy of Currently Used Paper Burn Diagram vs a Three-Dimensional Computerized Model.J Burn Care Res. 2017 Jan/Feb;38(1):e254-e260. doi: 10.1097/BCR.0000000000000363. J Burn Care Res. 2017. PMID: 27294858 Free PMC article.
-
Changing the Way We Think About Burn Size Estimation.J Burn Care Res. 2019 Jan 1;40(1):1-11. doi: 10.1093/jbcr/iry050. J Burn Care Res. 2019. PMID: 30247559 Review.
Cited by
-
3D PED BURN app: A precise and easy-to-use pediatric 3D burn surface area calculation tool.Health Sci Rep. 2022 Jun 16;5(4):e694. doi: 10.1002/hsr2.694. eCollection 2022 Jul. Health Sci Rep. 2022. PMID: 35755413 Free PMC article.
-
Utility of Telehealth Platforms Applied to Burns Management: A Systematic Review.Int J Environ Res Public Health. 2023 Feb 10;20(4):3161. doi: 10.3390/ijerph20043161. Int J Environ Res Public Health. 2023. PMID: 36833860 Free PMC article.
-
Early clinical management of severe burn patients using telemedicine: a pilot study protocol.Pilot Feasibility Stud. 2020 Jul 4;6:93. doi: 10.1186/s40814-020-00637-7. eCollection 2020. Pilot Feasibility Stud. 2020. PMID: 32637150 Free PMC article.
-
Telehealth and Burn Care: From Faxes to Augmented Reality.Bioengineering (Basel). 2022 May 13;9(5):211. doi: 10.3390/bioengineering9050211. Bioengineering (Basel). 2022. PMID: 35621489 Free PMC article.
-
Practical Computer Vision Application to Compute Total Body Surface Area Burn: Reappraising a Fundamental Burn Injury Formula in the Modern Era.JAMA Surg. 2022 Feb 1;157(2):129-135. doi: 10.1001/jamasurg.2021.5848. JAMA Surg. 2022. PMID: 34817552 Free PMC article.
References
-
- Hammond JS, Ward CG. Transfers from emergency room to burn center: Errors in burn size estimate. J Trauma. 1987;27:1161–5. - PubMed
-
- Nichter LS, Bryant CA, Edlich RF. Efficacy of burned surface area estimates calculated from charts–the need for a computerbased model. J Trauma. 1985;25:477–81. - PubMed
-
- Livingston EH, Lee S. Percentage of burned body surface area determination in obese and nonobese patients. J Surg Res. 2000;91:106–10. - PubMed
-
- Livingston EH, Lee S. Body surface area prediction in normalweight and obese patients. Am J Physiol Endocrinol Metab. 2001;281:586–91. - PubMed
-
- Verbraecken J, Van de HP, De BW, et al. Body surface area in normal-weight, overweight, and obese adults. A comparison study. Metabolism. 2006;55:515–24. - PubMed
LinkOut - more resources
Full Text Sources