

Management of Musculoskeletal Manifestations in Inflammatory Bowel Disease
- PMID: 26170832
- PMCID: PMC4478299
- DOI: 10.1155/2015/387891
Management of Musculoskeletal Manifestations in Inflammatory Bowel Disease
Abstract
Musculoskeletal manifestations are the most common extraintestinal manifestations in inflammatory bowel diseases. Some appendicular manifestations are independent of gut inflammation and are treated with standard anti-inflammatory strategies. On the other hand, axial involvement is linked to gut inflammatory activity; hence, there is a considerable amount of treatment overlap. Biological therapies have revolutionized management of inflammatory bowel diseases as well as of associated articular manifestations. Newer mechanisms driving gut associated arthropathy have surfaced in the past decade and have enhanced our interests in novel treatment targets. Introduction of biosimilar molecules is expected in the US market in the near future and will provide an opportunity for considerable cost savings on healthcare. A multidisciplinary approach involving a gastroenterologist, rheumatologist, and physical therapist is ideal for these patients.
Figures
Similar articles
-
The Impact of Inflammatory Bowel Disease in Canada 2018: Direct Costs and Health Services Utilization.J Can Assoc Gastroenterol. 2019 Feb;2(Suppl 1):S17-S33. doi: 10.1093/jcag/gwy055. Epub 2018 Nov 2. J Can Assoc Gastroenterol. 2019. PMID: 31294382 Free PMC article.
-
The joint-gut axis in inflammatory bowel diseases.J Crohns Colitis. 2010 Sep;4(3):257-68. doi: 10.1016/j.crohns.2009.11.005. Epub 2009 Nov 30. J Crohns Colitis. 2010. PMID: 21122514 Review.
-
IBD and arthropathies: a practical approach to its diagnosis and management.Gut. 2011 Oct;60(10):1426-35. doi: 10.1136/gut.2010.228866. Epub 2011 May 6. Gut. 2011. PMID: 21551189 Review.
-
Musculoskeletal manifestations of inflammatory bowel disease.Inflamm Bowel Dis. 2009 Dec;15(12):1915-24. doi: 10.1002/ibd.20942. Epub 2009 Apr 30. Inflamm Bowel Dis. 2009. PMID: 19408334 Review.
-
Paradoxical articular manifestations in patients with inflammatory bowel diseases treated with infliximab.Eur J Gastroenterol Hepatol. 2016 Aug;28(8):876-81. doi: 10.1097/MEG.0000000000000643. Eur J Gastroenterol Hepatol. 2016. PMID: 27101404
Cited by
-
Role of Biologic Therapies in the Rheumatic Manifestations of Inflammatory Bowel Disease: A Systematic Analysis.Cureus. 2023 Sep 13;15(9):e45195. doi: 10.7759/cureus.45195. eCollection 2023 Sep. Cureus. 2023. PMID: 37842480 Free PMC article. Review.
-
Status of etoricoxib in the treatment of rheumatic diseases. Expert panel opinion.Reumatologia. 2017;55(6):290-297. doi: 10.5114/reum.2017.72626. Epub 2017 Dec 30. Reumatologia. 2017. PMID: 29491537 Free PMC article. Review.
-
Inflammatory bowel diseases and spondyloarthropathies: From pathogenesis to treatment.World J Gastroenterol. 2019 May 14;25(18):2162-2176. doi: 10.3748/wjg.v25.i18.2162. World J Gastroenterol. 2019. PMID: 31143068 Free PMC article. Review.
-
Metabolic musculoskeletal disorders in patients with inflammatory bowel disease.Korean J Intern Med. 2025 Mar;40(2):181-195. doi: 10.3904/kjim.2024.359. Epub 2025 Mar 1. Korean J Intern Med. 2025. PMID: 40102707 Free PMC article. Review.
-
The shared circulating diagnostic biomarkers and molecular mechanisms of systemic lupus erythematosus and inflammatory bowel disease.Front Immunol. 2024 May 7;15:1354348. doi: 10.3389/fimmu.2024.1354348. eCollection 2024. Front Immunol. 2024. PMID: 38774864 Free PMC article.
References
-
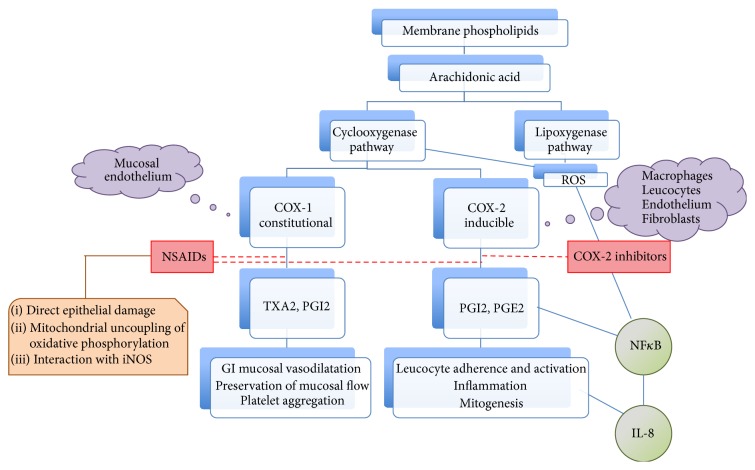
- Alzoghaibi M. A., Walsh S. W., Willey A., Yager D. R., Fowler A. A., III, Graham M. F. Linoleic acid induces interleukin-8 production by Crohn's human intestinal smooth muscle cells via arachidonic acid metabolites. The American Journal of Physiology—Gastrointestinal and Liver Physiology. 2004;286(4):G528–G537. doi: 10.1152/ajpgi.00189.2003. - DOI - PubMed
-
- Tanaka K.-I., Suemasu S., Ishihara T., Tasaka Y., Arai Y., Mizushima T. Inhibition of both COX-1 and COX-2 and resulting decrease in the level of prostaglandins E2 is responsible for non-steroidal anti-inflammatory drug (NSAID)-dependent exacerbation of colitis. European Journal of Pharmacology. 2009;603(1–3):120–132. doi: 10.1016/j.ejphar.2008.11.058. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
