

Apexification of an Immature Permanent Incisor with the Use of Calcium Hydroxide: 16-Year Follow-Up of a Case
- PMID: 26171256
- PMCID: PMC4480250
- DOI: 10.1155/2015/984590
Apexification of an Immature Permanent Incisor with the Use of Calcium Hydroxide: 16-Year Follow-Up of a Case
Abstract
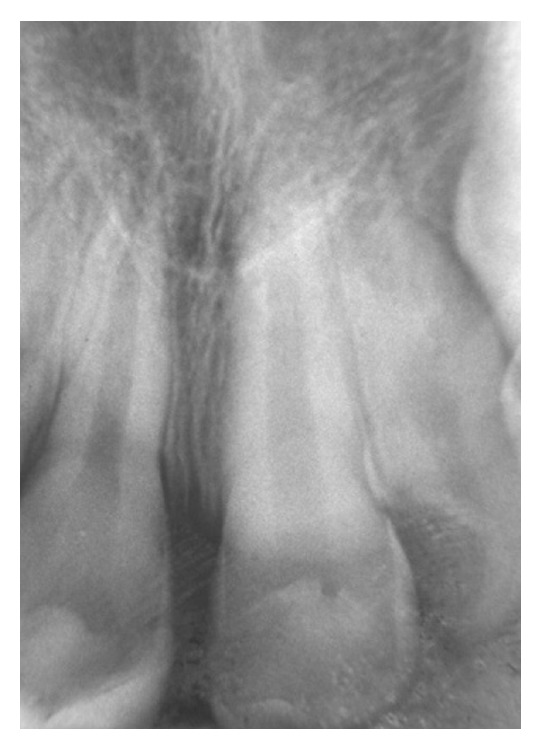
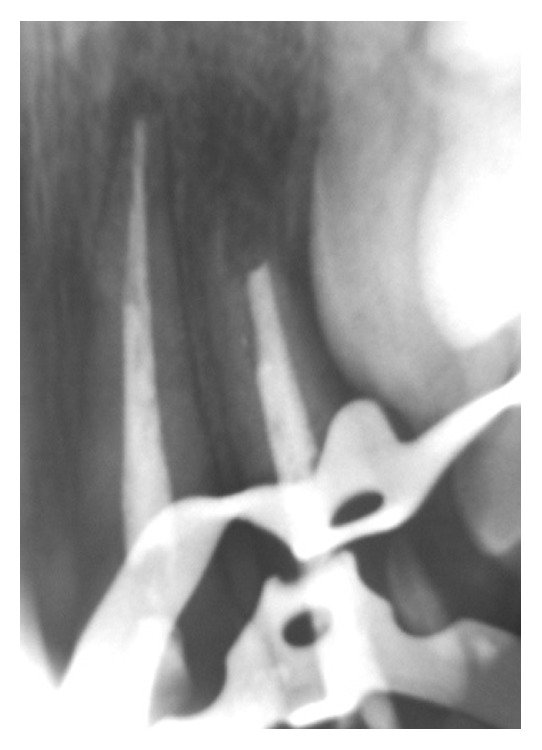
Apexification is a process of forming a mineralized apical barrier and had been performed by using calcium hydroxide paste, due to its biological and healing performances in cases of existent trauma. This clinical report aims to report the results of a 16-year follow-up study of an apexification treatment applied to nonvital tooth 22 of a healthy 8-year-old male after a trauma. Clinical inspection of the tooth showed fractures of the incisal edge and mesial angle, absence of coronal mobility, and negative pulp vitality under cold testing. Radiographic analysis of the root revealed incomplete apex formation. The possibility of fracture into the root or luxation injury was rejected, and the diagnosis of pulp necrosis was verified. Apexification by calcium hydroxide and subsequent endodontic treatment were planned. Initial formation of the mineralized apical barrier was observed after 3 months, and the barrier was considered to be completed after 8 months. Clinical, radiographic, and CBCT examinations after 16 years verified the success of the treatment, although the choice of calcium hydroxide for apexification treatment is discussed.
Figures







Similar articles
-
Calcium hydroxide induced apical barrier in fractured nonvital immature permanent incisors.J Indian Soc Pedod Prev Dent. 2010 Apr-Jun;28(2):110-2. doi: 10.4103/0970-4388.66750. J Indian Soc Pedod Prev Dent. 2010. PMID: 20660978
-
Duration for apical barrier formation in necrotic immature permanent incisors treated with calcium hydroxide apexification using ultrasonic or hand filing.J Formos Med Assoc. 2010 Aug;109(8):596-602. doi: 10.1016/S0929-6646(10)60097-6. J Formos Med Assoc. 2010. PMID: 20708511 Clinical Trial.
-
Induced post-traumatic apexification: 20 year follow-up and morphological study after new fracture.Ann Anat. 2018 Mar;216:120-124. doi: 10.1016/j.aanat.2017.12.005. Epub 2018 Jan 1. Ann Anat. 2018. PMID: 29301094
-
Apical Closure in Apexification: A Review and Case Report of Apexification Treatment of an Immature Permanent Tooth with Biodentine.J Endod. 2016 May;42(5):730-4. doi: 10.1016/j.joen.2016.02.007. Epub 2016 Mar 16. J Endod. 2016. PMID: 26994597 Review.
-
Use of calcium hydroxide for apical barrier formation and healing in non-vital immature permanent teeth: a review.Br Dent J. 1997 Oct 11;183(7):241-6. doi: 10.1038/sj.bdj.4809477. Br Dent J. 1997. PMID: 9364090 Review.
Cited by
-
Unusual foreign object in a tooth: A case report and review of literature.Clin Pract. 2019 Feb 11;9(1):1114. doi: 10.4081/cp.2019.1114. eCollection 2019 Jan 29. Clin Pract. 2019. PMID: 30881605 Free PMC article.
-
The effect of varying thicknesses of mineral trioxide aggregate (MTA) and Biodentine as apical plugs on the fracture resistance of teeth with simulated open apices: a comparative in vitro study.PeerJ. 2024 Dec 18;12:e18691. doi: 10.7717/peerj.18691. eCollection 2024. PeerJ. 2024. PMID: 39713144 Free PMC article.
-
Calcium sustained release, pH changes and cell viability induced by chitosan-based pastes for apexification.Odontology. 2019 Apr;107(2):223-230. doi: 10.1007/s10266-018-0389-7. Epub 2018 Sep 18. Odontology. 2019. PMID: 30229345
References
-
- Yassen G. H., Chin J., Mohammedsharif A. G., Alsoufy S. S., Othman S. S., Eckert G. The effect of frequency of calcium hydroxide dressing change and various pre- and inter-operative factors on the endodontic treatment of traumatized immature permanent incisors. Dental Traumatology. 2012;28(4):296–301. doi: 10.1111/j.1600-9657.2011.01089.x. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
