

Peroral endoscopic myotomy (POEM) vs laparoscopic Heller myotomy (LHM) for the treatment of Type III achalasia in 75 patients: a multicenter comparative study
- PMID: 26171430
- PMCID: PMC4486039
- DOI: 10.1055/s-0034-1391668
Peroral endoscopic myotomy (POEM) vs laparoscopic Heller myotomy (LHM) for the treatment of Type III achalasia in 75 patients: a multicenter comparative study
Abstract
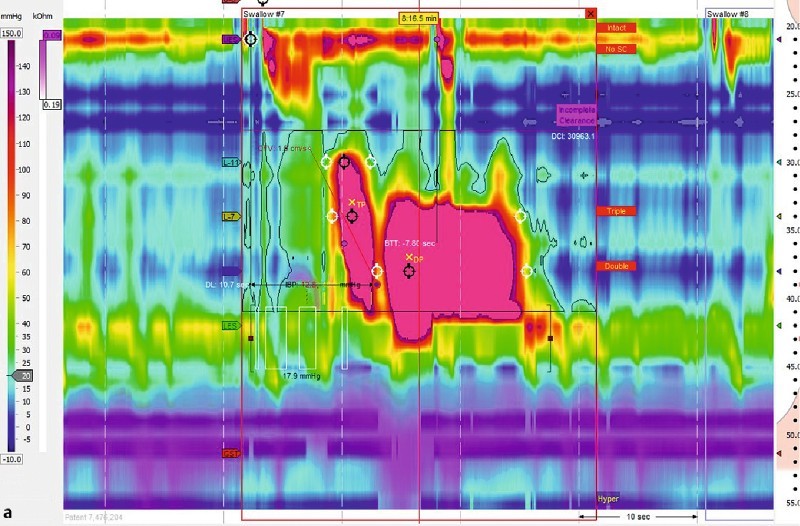
Background and study aims: Type III achalasia is characterized by rapidly propagating pressurization attributable to spastic contractions. Although laparoscopic Heller myotomy (LHM) is the current gold standard management for type III achalasia, peroral endoscopic myotomy (POEM) is conceivably superior because it allows for a longer myotomy. Our aims were to compare the efficacy and safety of POEM with LHM for type III achalasia patients.
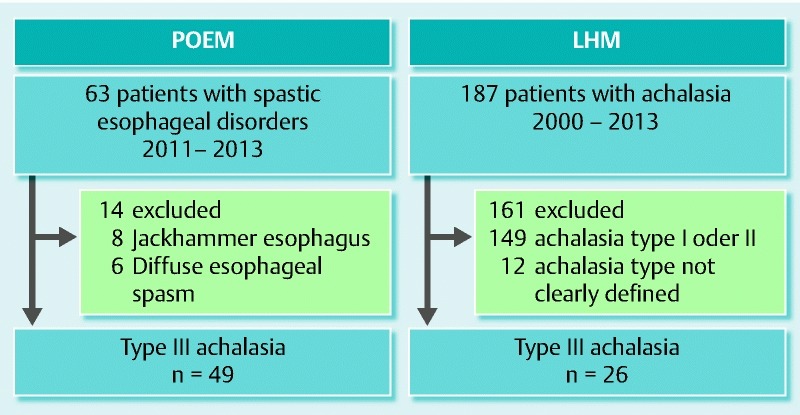
Patients and methods: A retrospective study of 49 patients who underwent POEM for type III achalasia across eight centers were compared to 26 patients who underwent LHM at a single institution. Procedural data were abstracted and pre- and post-procedural symptoms were recorded. Clinical response was defined by improvement of symptoms and decrease in Eckardt stage to ≤ 1. Secondary outcomes included length of myotomy, procedure duration, length of hospital stay, and rate of adverse events.
Results: Clinical response was significantly more frequent in the POEM cohort (98.0 % vs 80.8 %; P = 0.01). POEM patients had significantly shorter mean procedure time than LHM patients (102 min vs 264 min; P < 0.01) despite longer length of myotomy (16 cm vs 8 cm; P < 0.01). There was no significant difference between POEM and LHM in the length of hospital stay (3.3 days vs 3.2 days; P = 0.68), respectively. Rate of adverse events was significantly less in the POEM group (6 % vs 27 %; P < 0.01).
Conclusions: POEM allows for a longer myotomy than LHM, which may result in improved clinical outcomes. POEM appears to be an effective and safe alternative to LHM in patients with type III achalasia.
Conflict of interest statement
Figures
Similar articles
-
Direct cost variance analysis of peroral endoscopic myotomy vs heller myotomy for management of achalasia: A tertiary referral center experience.World J Gastrointest Endosc. 2023 Oct 16;15(10):593-601. doi: 10.4253/wjge.v15.i10.593. World J Gastrointest Endosc. 2023. PMID: 37900115 Free PMC article.
-
Clinical and financial outcomes of per-oral endoscopic myotomy compared to laparoscopic heller myotomy for treatment of achalasia.Surg Endosc. 2023 Jul;37(7):5526-5537. doi: 10.1007/s00464-022-09652-6. Epub 2022 Oct 11. Surg Endosc. 2023. PMID: 36220985
-
Per Oral Endoscopic Myotomy (POEM) for pediatric achalasia: Institutional experience and outcomes.J Pediatr Surg. 2022 Nov;57(11):728-735. doi: 10.1016/j.jpedsurg.2022.02.017. Epub 2022 Feb 25. J Pediatr Surg. 2022. PMID: 35361482
-
Systematic Review and Meta-Analysis of Perioperative Outcomes of Peroral Endoscopic Myotomy (POEM) and Laparoscopic Heller Myotomy (LHM) for Achalasia.Surg Laparosc Endosc Percutan Tech. 2017 Jun;27(3):123-131. doi: 10.1097/SLE.0000000000000402. Surg Laparosc Endosc Percutan Tech. 2017. PMID: 28472017
-
Laparoscopic Heller Myotomy Versus Peroral Endoscopic Myotomy (POEM) for Achalasia: A Systematic Review and Meta-analysis.Ann Surg. 2018 Mar;267(3):451-460. doi: 10.1097/SLA.0000000000002311. Ann Surg. 2018. PMID: 28549006
Cited by
-
Symptom duration is not associated with per oral endoscopic myotomy (POEM) failure.Surg Endosc. 2023 Oct;37(10):8000-8005. doi: 10.1007/s00464-023-10253-0. Epub 2023 Jul 17. Surg Endosc. 2023. PMID: 37460816
-
2019 Seoul Consensus on Esophageal Achalasia Guidelines.J Neurogastroenterol Motil. 2020 Apr 30;26(2):180-203. doi: 10.5056/jnm20014. J Neurogastroenterol Motil. 2020. PMID: 32235027 Free PMC article. Review.
-
Expanding Role of Third Space Endoscopy in the Management of Esophageal Diseases.Curr Treat Options Gastroenterol. 2018 Mar;16(1):41-57. doi: 10.1007/s11938-018-0169-z. Curr Treat Options Gastroenterol. 2018. PMID: 29435819 Review.
-
Pre-treatment Eckardt score is a simple factor for predicting one-year peroral endoscopic myotomy failure in patients with achalasia.Surg Endosc. 2017 Aug;31(8):3234-3241. doi: 10.1007/s00464-016-5352-5. Epub 2016 Nov 18. Surg Endosc. 2017. PMID: 27864723
-
Cost-effectiveness of per oral endoscopic myotomy relative to laparoscopic Heller myotomy for the treatment of achalasia.Surg Endosc. 2018 Jan;32(1):39-45. doi: 10.1007/s00464-017-5629-3. Epub 2017 Dec 7. Surg Endosc. 2018. PMID: 29218664
References
-
- Boeckxstaens G, Zaninotto G. Achalasia and esophago-gastric junction outflow obstruction: focus on the subtypes. Neurogastroenterol Motil. 2012;24 01:27–31. - PubMed
-
- Moonen A, Boeckxstaens G. Current diagnosis and management of achalasia. J Clin Gastroenterol. 2014;48:484–490. - PubMed
-
- Patti M G Pellegrini C A Arcerito M et al.Comparison of medical and minimally invasive surgical therapy for primary esophageal motility disorders Arch Surg 1995130609–615.; discussion 615–616 - PubMed
-
- Salvador R, Costantini M, Zaninotto G. et al.The preoperative manometric pattern predicts the outcome of surgical treatment for esophageal achalasia. Journal of gastrointestinal surgery. J Gastrointest Surg. 2010;14:1635–1645. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources