

Relationship between indeterminate or positive lateral margin and local recurrence after endoscopic resection of colorectal polyps
- PMID: 26171439
- PMCID: PMC4486031
- DOI: 10.1055/s-0034-1391853
Relationship between indeterminate or positive lateral margin and local recurrence after endoscopic resection of colorectal polyps
Abstract
Background and study aims: Although endoscopic resection is widely used for the treatment of superficial colorectal neoplasms, the rate of local recurrence of lesions with a positive or indeterminate lateral margin on histologic evaluation is unclear. We aimed to demonstrate the relationship between lateral margin status and local recurrence after the endoscopic resection of intramucosal colorectal neoplasms.
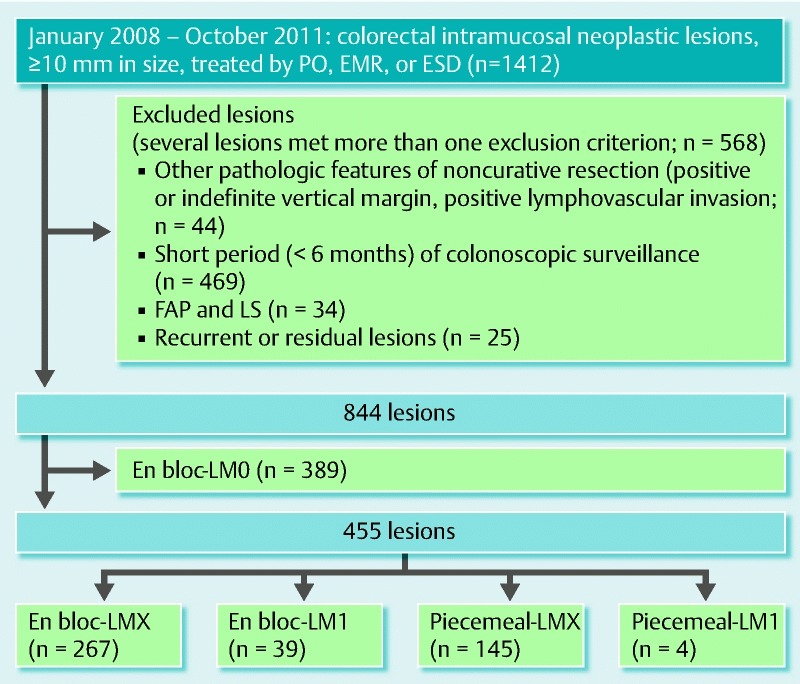
Patients and methods: We retrospectively collected the clinical and pathologic data for 844 endoscopically resected colorectal intramucosal neoplasms with a size of 10 mm or larger. We investigated the relationship between the local recurrence rate and the lateral margin status (categorized as LM0 [negative], LM1 [positive], or LMX [indeterminate]).
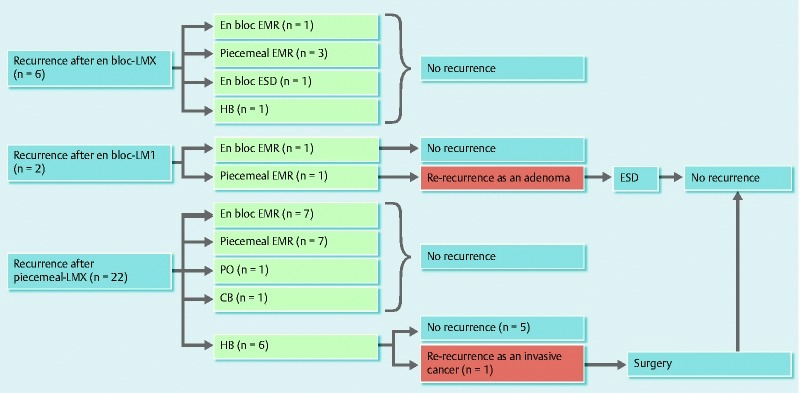
Results: In total, 389 lesions were evaluated as LM0 and showed no local recurrence. Of the 455 lesions evaluated as LMX or LM1, 30 showed local recurrence within a median period of 6.3 months (range, 1.7 - 48.1) from the initial endoscopic resection. The local recurrence rate of the en bloc-LMX group (2.2 %) was significantly lower than that of the piecemeal-LMX group (15.2 %). Of the 30 cases of recurrence, 28 were successfully treated with a second endoscopic resection. Of the two lesions that showed further recurrence, one was treated with a third endoscopic resection, whereas the other - which was a piecemeal-LMX lesion - was eventually diagnosed as invasive cancer and treated with surgery.
Conclusions: The local recurrence rate was lower in the en bloc-LMX group than in the piecemeal-LMX group. Thus, we believe that en bloc-LMX lesions that are completely and confidently resected endoscopically can be treated as en bloc-LM0 lesions.
Conflict of interest statement
Figures
Similar articles
-
Recurrence rate of lateral margin-positive cases after en bloc endoscopic submucosal dissection of colorectal neoplasia.Int J Colorectal Dis. 2018 Jun;33(6):735-743. doi: 10.1007/s00384-018-3012-z. Epub 2018 Mar 12. Int J Colorectal Dis. 2018. PMID: 29532207
-
The relationship between local recurrence and positive lateral margin after en bloc resection of colorectal neoplasm.Scand J Gastroenterol. 2018 Dec;53(12):1541-1546. doi: 10.1080/00365521.2018.1547419. Epub 2019 Jan 2. Scand J Gastroenterol. 2018. PMID: 30600737
-
Local recurrence after endoscopic resection of colorectal tumors.Int J Colorectal Dis. 2009 Feb;24(2):225-30. doi: 10.1007/s00384-008-0596-8. Epub 2008 Oct 30. Int J Colorectal Dis. 2009. PMID: 18972121
-
AGA Institute Clinical Practice Update: Endoscopic Submucosal Dissection in the United States.Clin Gastroenterol Hepatol. 2019 Jan;17(1):16-25.e1. doi: 10.1016/j.cgh.2018.07.041. Epub 2018 Aug 2. Clin Gastroenterol Hepatol. 2019. PMID: 30077787 Review.
-
Our perspective on endoscopic resection for colorectal neoplasms.Gastroenterol Clin Biol. 2010 Aug-Sep;34(6-7):367-70. doi: 10.1016/j.gcb.2010.05.002. Epub 2010 Jun 23. Gastroenterol Clin Biol. 2010. PMID: 20576382 Review.
Cited by
-
The influence of adjuvant therapy on survival in patients with indeterminate margins following surgery for non-small cell lung cancer.J Thorac Cardiovasc Surg. 2020 May;159(5):2030-2040.e4. doi: 10.1016/j.jtcvs.2019.09.075. Epub 2019 Sep 30. J Thorac Cardiovasc Surg. 2020. PMID: 31706554 Free PMC article.
-
Low risk of local recurrence after a successful en bloc endoscopic submucosal dissection for noninvasive colorectal lesions with positive horizontal resection margins (R-ESD study).Endoscopy. 2023 Mar;55(3):245-251. doi: 10.1055/a-1960-3552. Epub 2022 Oct 13. Endoscopy. 2023. PMID: 36228648 Free PMC article.
-
Recurrence with malignancy after endoscopic resection of large colon polyps with high-grade dysplasia: incidence and risk factors.Surg Endosc. 2021 Jun;35(6):2500-2508. doi: 10.1007/s00464-020-07660-y. Epub 2020 May 29. Surg Endosc. 2021. PMID: 32472496
-
Colorectal polyps located across a fold are difficult to resect completely using endoscopic mucosal resection: A propensity score analysis.United European Gastroenterol J. 2018 Dec;6(10):1547-1555. doi: 10.1177/2050640618797854. Epub 2018 Aug 24. United European Gastroenterol J. 2018. PMID: 30574325 Free PMC article.
-
Clinical feasibility of endoscopic submucosal dissection with minimum lateral margin of superficial esophageal squamous cell carcinoma.Endosc Int Open. 2019 Apr;7(4):E396-E402. doi: 10.1055/a-0838-5064. Epub 2019 Mar 15. Endosc Int Open. 2019. PMID: 30931369 Free PMC article.
References
-
- Deyhle P, Seuberth K, Jenny S. et al.Endoscopic polypectomy in the proximal colon. Endoscopy. 1971;3:103–115.
-
- Deyhle P, Largiader F, Fumagalli S. A method for endoscopic electroresection of sessile colonic polyps. Endoscopy. 1973;5:38–40.
-
- Kudo S. Endoscopic mucosal resection of flat and depressed type of early colorectal cancer. Endoscopy. 1993;25:455–461. - PubMed
-
- Ahmad N A, Kochman M L, Long W B. et al.Efficacy, safety, and clinical outcomes of endoscopic mucosal resection: a study of 101 cases. Gastrointest Endosc. 2002;55:390–396. - PubMed
-
- Moss A, Bourke M J, Williams S J. et al.Endoscopic mucosal resection outcomes and prediction of submucosal cancer from advanced colonic mucosal neoplasia. Gastroenterology. 2011;140:1909–1918. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials