

Impact of p16 status on pro- and anti-angiogenesis factors in head and neck cancers
- PMID: 26171937
- PMCID: PMC4647678
- DOI: 10.1038/bjc.2015.251
Impact of p16 status on pro- and anti-angiogenesis factors in head and neck cancers
Abstract
Background: Head and neck cancers (HNC) are aggressive tumours. Overexpression of p16 in HNC correlates with human papilloma virus (HPV)-associated HNC that carry a better prognosis than HPV-negative tumours. Angiogenesis is an important factor in tumour progression. Our aim was to dissect the impact of p16 expression on angiogenesis factors in HNC.
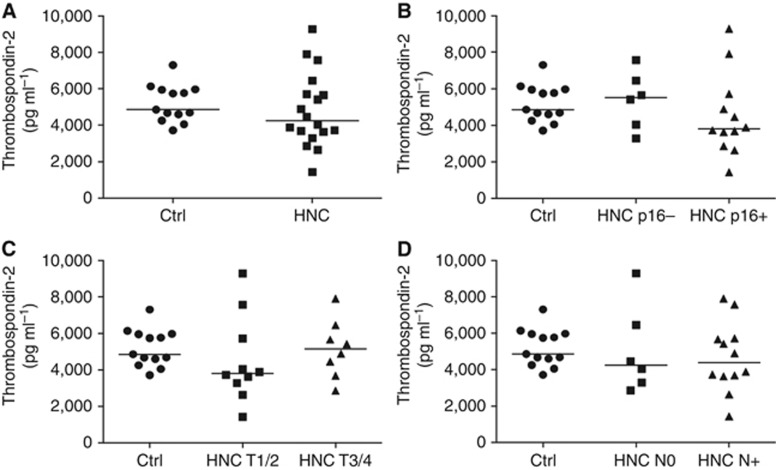
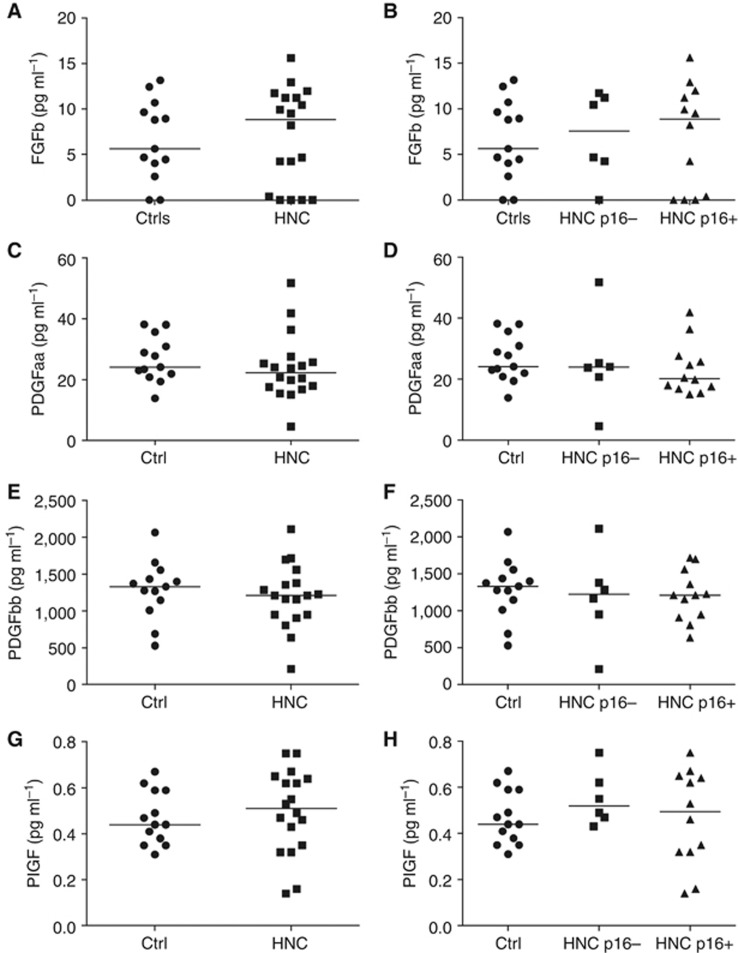
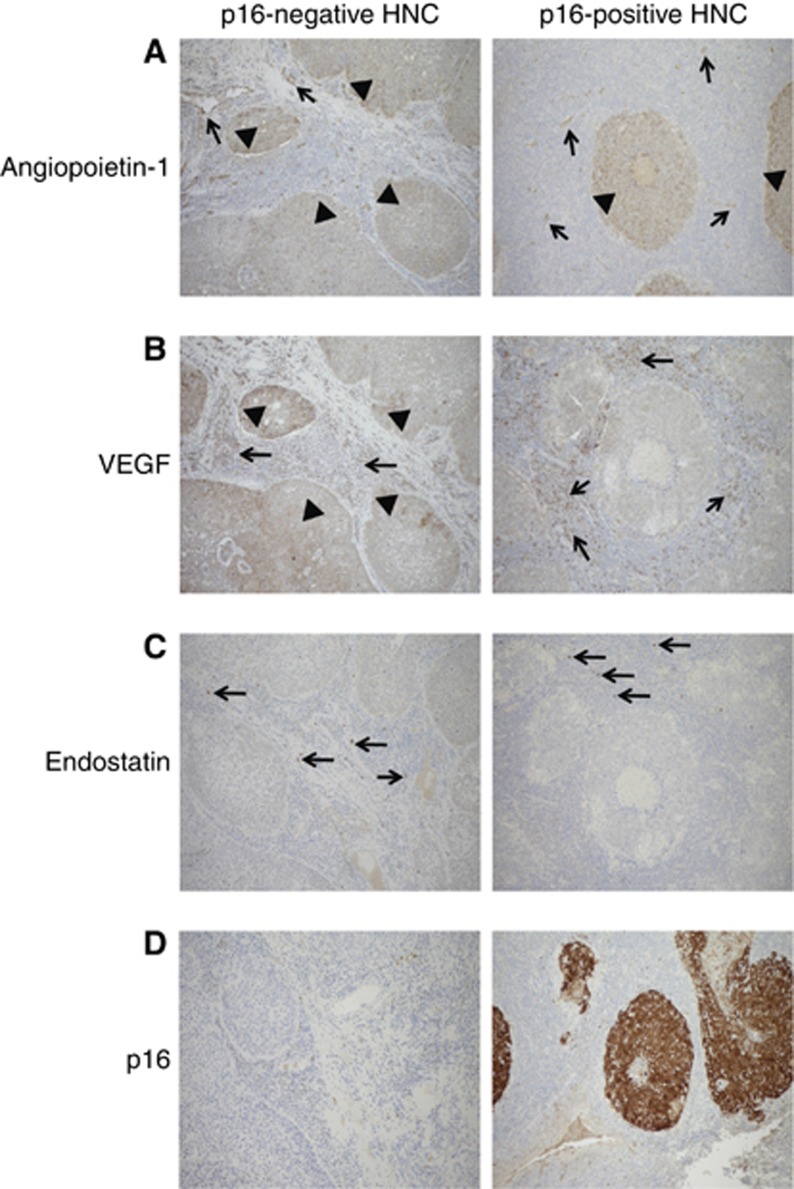
Methods: Eighteen newly diagnosed HNC patients and controls were analysed. Eleven pro- and anti-angiogenesis factors were quantified using multiplex ELISA in HNC patients and controls. Angiogenesis factors were analysed in tumour tissue using immunohistochemistry.
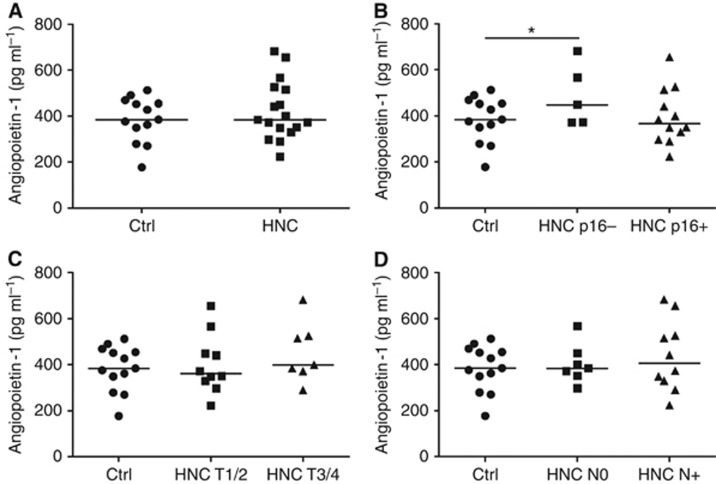
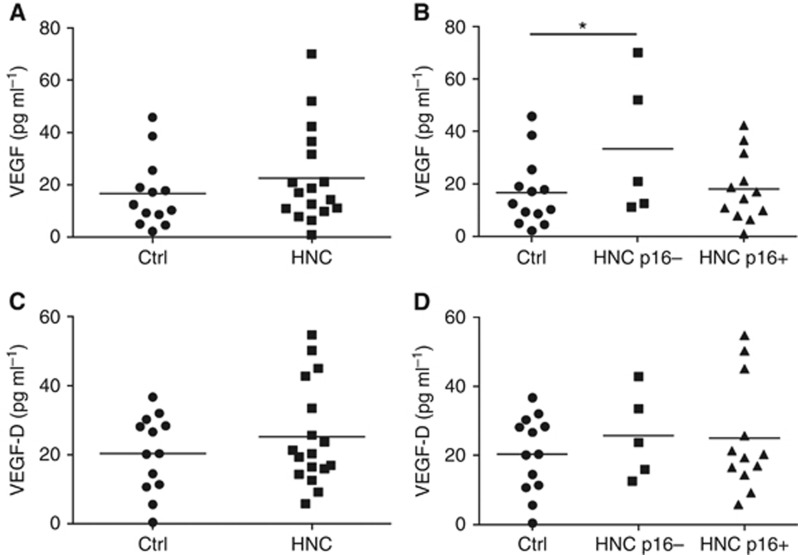
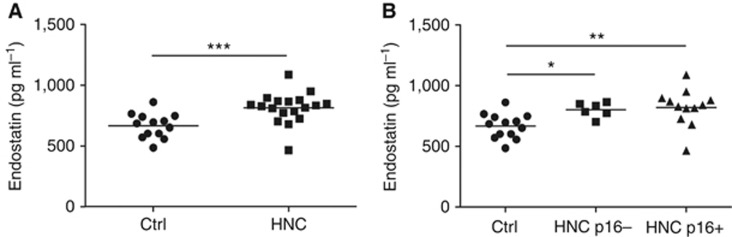
Results: Circulating levels of endostatin (anti-angiogenesis factor) were higher in the HNC group compared with healthy donors. Interestingly, the pro-angiogenesis factors angiopoietin-1 and vascular endothelial growth factor (VEGF) were significantly higher in patients with p16-negative compared with p16-positive HNC. Moreover, the major source of VEGF in p16-positive HNC tissue was tumour stromal cells. In contrast, both tumour cells and stromal cells expressed VEGF in p16-negative tissue.
Conclusions: We show that p16-negative tumours associate with increased circulating levels of pro-angiogenic VEGF and angiopoietin-1. Tissue expression of VEGF differs between p16-positive and p16-negative tumours. These findings may explain differences in the biological behaviour of p16-positive and p16-negative HNC. Better understanding of mechanisms by which the p16 status influences tumour angiogenesis may guide the development of targeted therapies.
Figures
References
-
- Blezinger P, Wang J, Gondo M, Quezada A, Mehrens D, French M, Singhal A, Sullivan S, Rolland A, Ralston R, Min W (1999) Systemic inhibition of tumor growth and tumor metastases by intramuscular administration of the endostatin gene. Nat Biotechnol 17(4): 343–348. - PubMed
-
- Cohen EE, Davis DW, Karrison TG, Seiwert TY, Wong SJ, Nattam S, Kozloff MF, Clark JI, Yan DH, Liu W, Pierce C, Dancey JE, Stenson K, Blair E, Dekker A, Vokes EE (2009) Erlotinib and bevacizumab in patients with recurrent or metastatic squamous-cell carcinoma of the head and neck: a phase I/II study. Lancet Oncol 10(3): 247–257. - PMC - PubMed
-
- Ferrara N, Davis-Smyth T (1997) The biology of vascular endothelial growth factor. Endocr Rev 18(1): 4–25. - PubMed
-
- Folkman J, Watson K, Ingber D, Hanahan D (1989) Induction of angiogenesis during the transition from hyperplasia to neoplasia. Nature 339(6219): 58–61. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
