

Calcium Disorders in the Emergency Department: Independent Risk Factors for Mortality
- PMID: 26172117
- PMCID: PMC4501826
- DOI: 10.1371/journal.pone.0132788
Calcium Disorders in the Emergency Department: Independent Risk Factors for Mortality
Abstract
Background: Calcium disorders are common in both intensive care units and in patients with chronic kidney disease and are associated with increased morbidity and mortality. It is unknown whether calcium abnormalities in unselected emergency department admissions have an impact on in-hospital mortality.
Methods: This cross-sectional analysis included all admissions to the Emergency Department at the Inselspital Bern, Switzerland from 2010 to 2011. For hyper- and hypocalcaemic patients with a Mann-Whitney U-test, the differences between subgroups divided by age, length of hospital stay, creatinine, sodium, chloride, phosphate, potassium and magnesium were compared. Associations between calcium disorders and 28-day in-hospital mortality were assessed using the Cox proportional hazard regression model.
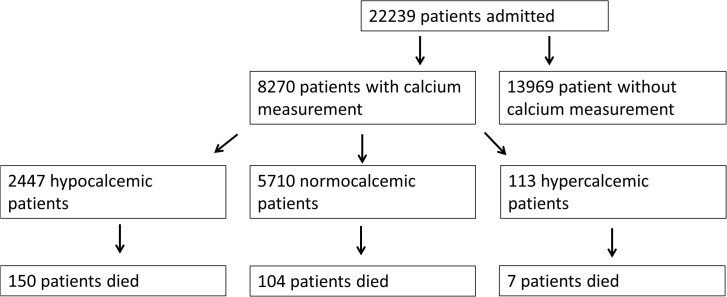
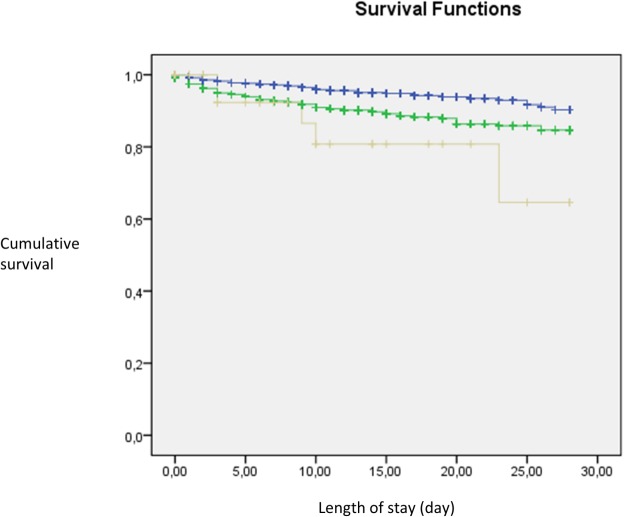
Results: 8,270 patients with calcium measurements were included in our study. Overall 264 (3.2%) patients died. 150 patients (6.13%) with hypocalcaemia and 7 patients with hypercalcaemia (6.19%) died, in contrast to 104 normocalcaemic patients (1.82%). In univariate analysis, calcium serum levels were associated with sex, mortality and pre-existing diuretic therapy (all p<0.05). In multivariate Cox regression analysis, hypocalcaemia and hypercalcaemia were independent risk factors for mortality (HR 2.00 and HR 1.88, respectively; both p<0.01).
Conclusion: Both hypocalcaemia and hypercalcaemia are associated with increased 28-day in-hospital mortality in unselected emergency department admissions.
Conflict of interest statement
Figures
References
-
- Lee CT, Yang CC, Lam KK, Kung CT, Tsai CJ, Chen HC. Hypercalcemia in the emergency department. Am J Med Sci 2006;331:119–123. - PubMed
-
- Zivin JR, Gooley T, Zager RA, Ryan MJ. Hypocalcemia: a pervasive metabolic abnormality in the critically ill. Am J Kidney Dis 2001;37:689–698. - PubMed
-
- Desai TK, Carlson RW, Geheb MA. Prevalence and clinical implications of hypocalcemia in acutely ill patients in a medical intensive care setting. Am J Med 1988;84:209–214. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
