

Altered Resting-State Connectivity within Executive Networks after Aneurysmal Subarachnoid Hemorrhage
- PMID: 26172281
- PMCID: PMC4501762
- DOI: 10.1371/journal.pone.0130483
Altered Resting-State Connectivity within Executive Networks after Aneurysmal Subarachnoid Hemorrhage
Abstract
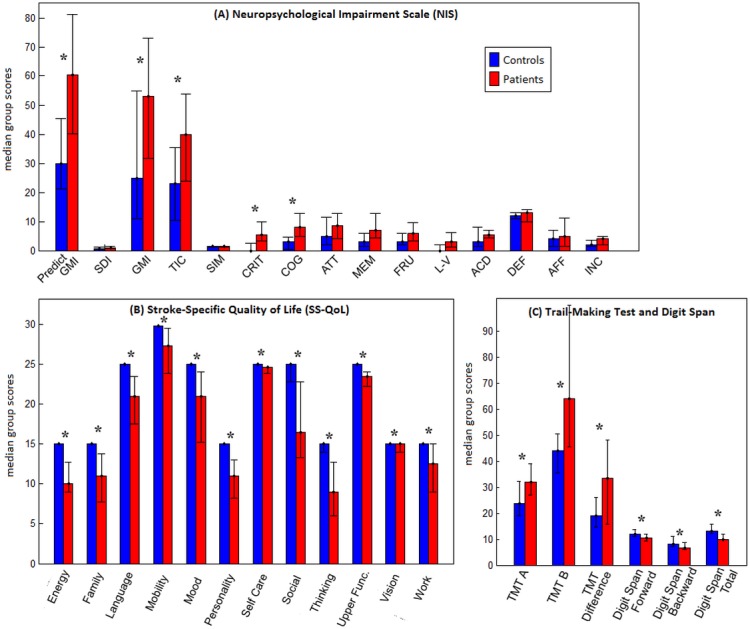
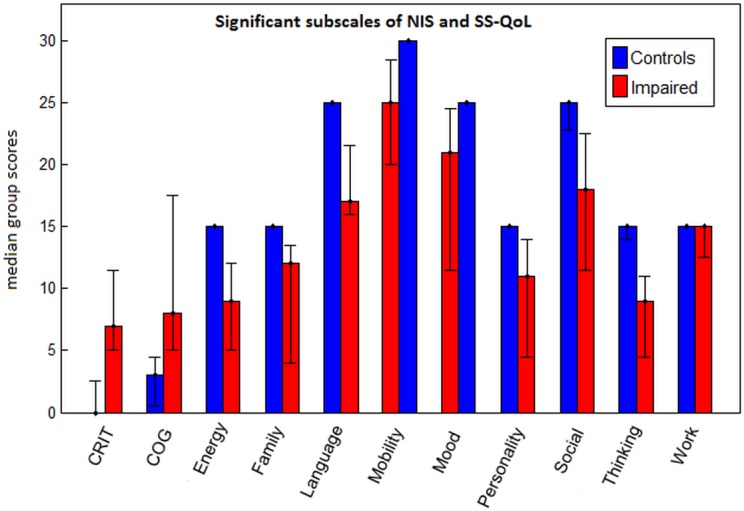
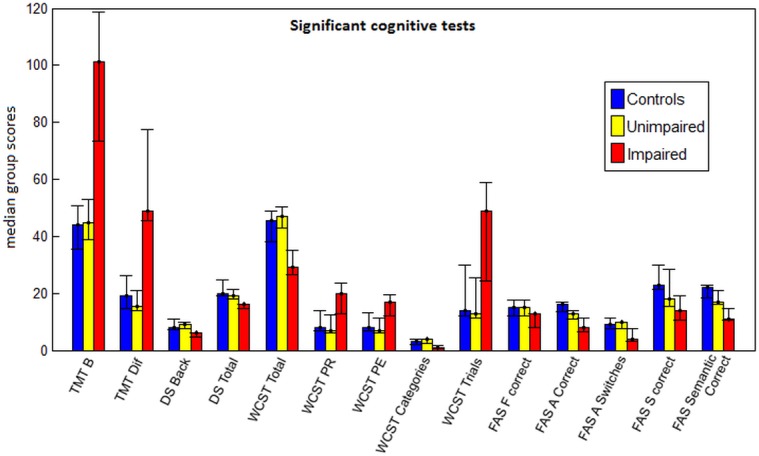
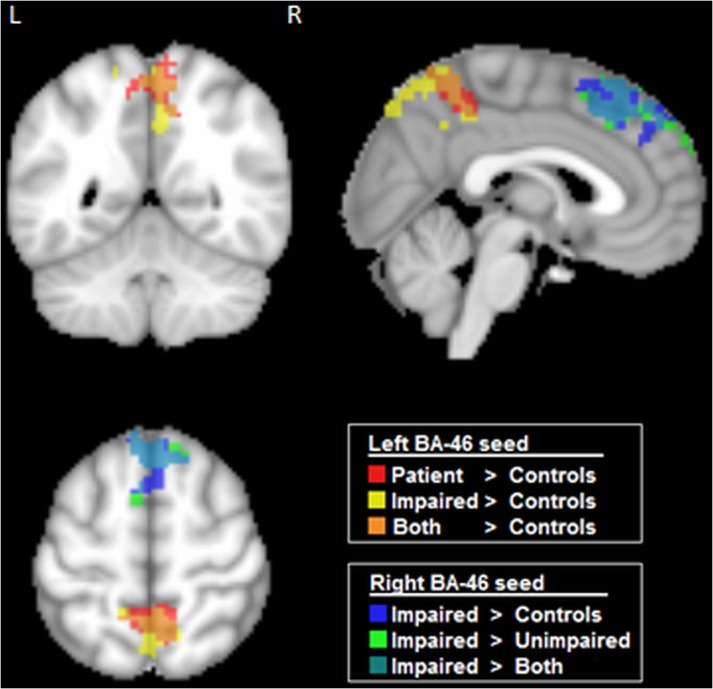
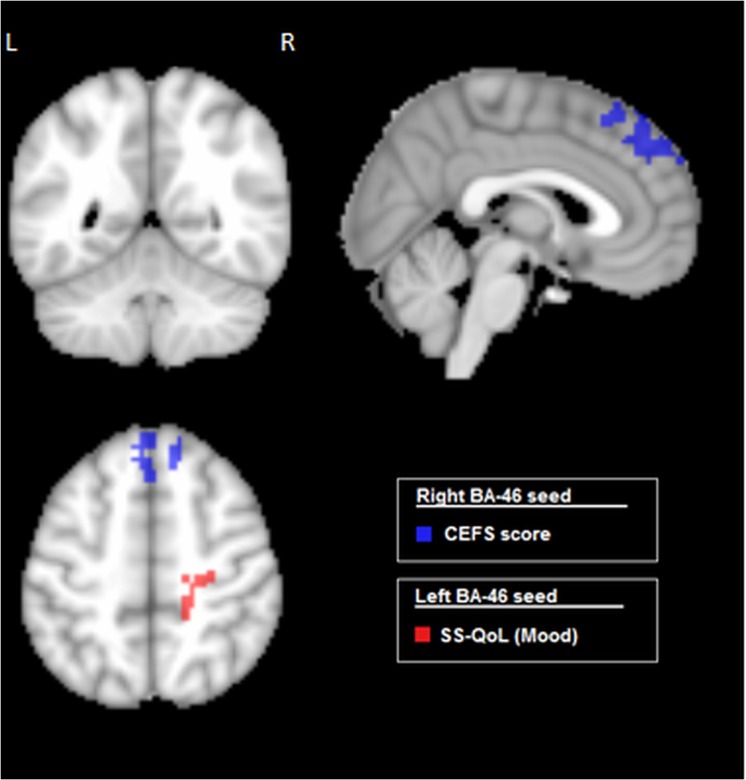
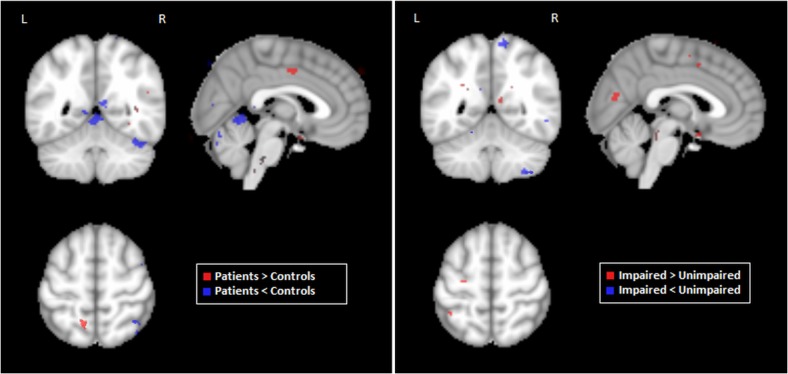
Aneurysmal subarachnoid hemorrhage (aSAH) is associated with significant mortality rates, and most survivors experience significant cognitive deficits across multiple domains, including executive function. It is critical to determine the neural basis for executive deficits in aSAH, in order to better understand and improve patient outcomes. This study is the first examination of resting-state functional Magnetic Resonance Imaging in a group of aSAH patients, used to characterize changes in functional connectivity of the frontoparietal network. We scanned 14 aSAH patients and 14 healthy controls, and divided patients into "impaired" and "unimpaired" groups based on a composite executive function score. Impaired patients exhibited significantly lower quality of life and neuropsychological impairment relative to controls, across multiple domains. Seed-based functional connectivity analysis demonstrated that unimpaired patients were not significantly different from controls, but impaired patients had increased frontoparietal connectivity. Patients evidenced increased frontoparietal connectivity as a function of decreased executive function and decreased mood (i.e. quality of life). In addition, T1 morphometric analysis demonstrated that these changes are not attributable to local cortical atrophy among aSAH patients. These results establish significant, reliable changes in the endogenous brain dynamics of aSAH patients, that are related to cognitive and mood outcomes.
Conflict of interest statement
Figures
Similar articles
-
Memory Deficits After Aneurysmal Subarachnoid Hemorrhage: A Functional Magnetic Resonance Imaging Study.World Neurosurg. 2018 Mar;111:e500-e506. doi: 10.1016/j.wneu.2017.12.102. Epub 2017 Dec 26. World Neurosurg. 2018. PMID: 29288107
-
Impaired Work Productivity After Aneurysmal Subarachnoid Hemorrhage.J Neurosci Nurs. 2016 Oct;48(5):260-8. doi: 10.1097/JNN.0000000000000209. J Neurosci Nurs. 2016. PMID: 27579960 Free PMC article.
-
Cognitive and functional outcome after aneurysmal subarachnoid hemorrhage.Stroke. 2010 Aug;41(8):e519-36. doi: 10.1161/STROKEAHA.110.581975. Epub 2010 Jul 1. Stroke. 2010. PMID: 20595669 Review.
-
Altered resting-state functional organization within the central executive network in obsessive-compulsive disorder.Psychiatry Clin Neurosci. 2016 Oct;70(10):448-456. doi: 10.1111/pcn.12419. Epub 2016 Aug 28. Psychiatry Clin Neurosci. 2016. PMID: 27377579
-
Neurocognitive outcomes after aneurysmal subarachnoid hemorrhage: Identifying inflammatory biomarkers.J Neurol Sci. 2018 Nov 15;394:84-93. doi: 10.1016/j.jns.2018.06.021. Epub 2018 Jun 25. J Neurol Sci. 2018. PMID: 30240942 Review.
Cited by
-
Magnetic Resonance Imaging in Aneurysmal Subarachnoid Hemorrhage: Current Evidence and Future Directions.Neurocrit Care. 2018 Oct;29(2):241-252. doi: 10.1007/s12028-018-0534-8. Neurocrit Care. 2018. PMID: 29633155
-
Subarachnoid hemorrhage leads to early and persistent functional connectivity and behavioral changes in mice.J Cereb Blood Flow Metab. 2021 May;41(5):975-985. doi: 10.1177/0271678X20940152. Epub 2020 Sep 16. J Cereb Blood Flow Metab. 2021. PMID: 32936728 Free PMC article.
-
Altered functional connectivity within default mode network after rupture of anterior communicating artery aneurysm.Front Aging Neurosci. 2022 Jul 25;14:905453. doi: 10.3389/fnagi.2022.905453. eCollection 2022. Front Aging Neurosci. 2022. PMID: 35959287 Free PMC article.
-
SIRT1 mediates hypoxic postconditioning- and resveratrol-induced protection against functional connectivity deficits after subarachnoid hemorrhage.J Cereb Blood Flow Metab. 2022 Jul;42(7):1210-1223. doi: 10.1177/0271678X221079902. Epub 2022 Feb 9. J Cereb Blood Flow Metab. 2022. PMID: 35137611 Free PMC article.
-
Clinical Factors Contributing to Cognitive Function in the Acute Stage after Treatment of Intracranial Aneurysms: A Cross-Sectional Study.J Clin Med. 2022 Aug 28;11(17):5053. doi: 10.3390/jcm11175053. J Clin Med. 2022. PMID: 36078981 Free PMC article.
References
-
- Hop J., Rinkel G., Algra A. and van Gijn J., "Case-fatality rates and functional outcome after subarachnoid hemorrhage: a systematic review," Stroke, vol. 28, no. 3, p. 660–664, 1997. - PubMed
-
- Hackett M. and Anderson C., "Health outcomes 1 year after subarachnoid hemorrhage: An international population-based study," Neurology, vol. 55, pp. 658–662, 2000. - PubMed
-
- Egge A., Waterloo K., Sjøholm H., Ingebrigtsen T., Forsdahl S., Jacobsen E. and Romner B., "utcome 1 year after aneurysmal subarachnoid hemorrhage: relation between cognitive performance and neuroimaging," Acta Neurologica Scandinavica, vol. 112, no. 2, p. 76–80, 2005. - PubMed
-
- Tidswell P., Dias P., Sagar H., Mayes A. and Battersby R., "Cognitive outcome after aneurysm rupture : Relationship to aneurysm site and perioperative complications.," Neurology, vol. 45, p. 875–882, 1995. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
