

Independent Determinants of Maternal and Fetal Outcomes in a Sample of Pregnant Outpatients With Normal Blood Pressure, Chronic Hypertension, Gestational Hypertension, and Preeclampsia
- PMID: 26173048
- PMCID: PMC8031729
- DOI: 10.1111/jch.12614
Independent Determinants of Maternal and Fetal Outcomes in a Sample of Pregnant Outpatients With Normal Blood Pressure, Chronic Hypertension, Gestational Hypertension, and Preeclampsia
Abstract
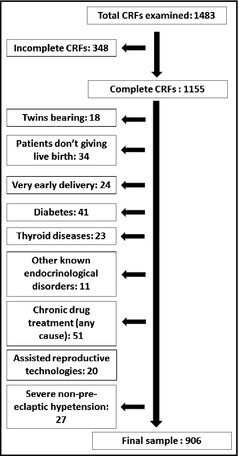
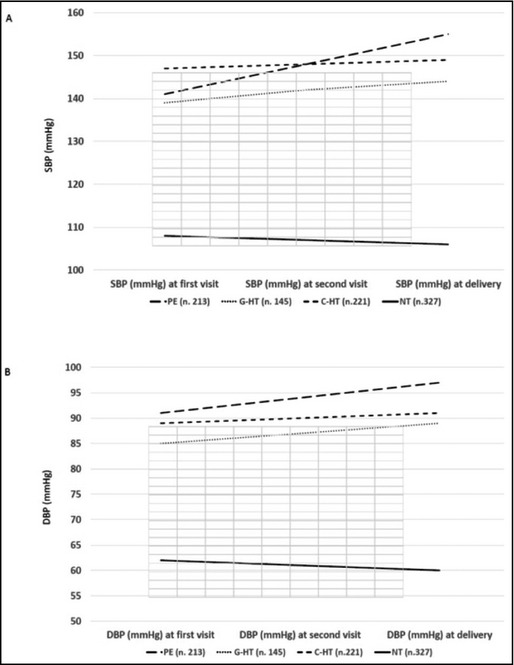
The aim of this retrospective study was to evaluate the main independent prognostic factors of negative maternal and fetal outcomes in a relatively large sample of pregnant outpatients (N=906) who were normotensive or affected by chronic hypertension, gestational hypertension, or preeclampsia. Among the studied parameters, the ones significantly associated with negative maternal outcomes were a diagnosis of preeclampsia (vs other forms of hypertension or normotension) and higher serum uric acid level, while antihypertensive treatment, number of previous deliveries, and blood pressure (BP) control at deliveries seemed to be protective. Regarding negative fetal outcomes, the parameters significantly associated with a negative maternal outcome were a diagnosis of preeclampsia (vs other forms of hypertension or normotension) and mother pre-pregnancy body mass index, while antihypertensive treatment and BP control at delivery seemed to be protective. Specific patient characteristics should help to predict the risk of negative maternal and fetal outcomes.
© 2015 Wiley Periodicals, Inc.
Figures
Comment in
-
Maternal and Fetal Outcomes in Preeclampsia: Interrelations Between Insulin Resistance, Aldosterone, Metabolic Syndrome, and Polycystic Ovary Syndrome.J Clin Hypertens (Greenwich). 2015 Oct;17(10):783-5. doi: 10.1111/jch.12613. Epub 2015 Jul 14. J Clin Hypertens (Greenwich). 2015. PMID: 26172964 Free PMC article. No abstract available.
Similar articles
-
Association of uric acid with progression to preeclampsia and development of adverse conditions in gestational hypertensive pregnancies.Am J Hypertens. 2012 Jun;25(6):711-7. doi: 10.1038/ajh.2012.18. Epub 2012 Mar 1. Am J Hypertens. 2012. PMID: 22378034
-
Maternal Serum Uric Acid as a Predictor of Severity of Hypertensive Disorders of Pregnancy: A Prospective Cohort Study.Curr Hypertens Rev. 2019;15(2):154-160. doi: 10.2174/1573402114666181112141953. Curr Hypertens Rev. 2019. PMID: 30417791 Free PMC article.
-
Prognostic significance of serum uric acid in women with gestational hypertension.Hypertension. 2011 Oct;58(4):704-8. doi: 10.1161/HYPERTENSIONAHA.111.177212. Epub 2011 Aug 29. Hypertension. 2011. PMID: 21876075
-
Prevention and treatment of pregnancy-associated hypertension: what have we learned in the last 10 years?Am J Kidney Dis. 1991 Sep;18(3):285-305. doi: 10.1016/s0272-6386(12)80087-4. Am J Kidney Dis. 1991. PMID: 1882820 Review.
-
The association between first trimester blood pressure, blood pressure trajectory, mid-pregnancy blood pressure drop and maternal and fetal outcomes: A systematic review and meta-analysis.Pregnancy Hypertens. 2024 Dec;38:101164. doi: 10.1016/j.preghy.2024.101164. Epub 2024 Oct 16. Pregnancy Hypertens. 2024. PMID: 39418860
Cited by
-
Hypertension in CKD Pregnancy: a Question of Cause and Effect (Cause or Effect? This Is the Question).Curr Hypertens Rep. 2016 Apr;18(5):35. doi: 10.1007/s11906-016-0644-7. Curr Hypertens Rep. 2016. PMID: 27072828 Review.
-
Association between Serum Uric Acid Levels and Perinatal Outcome in Women with Preeclampsia.Obstet Gynecol Int. 2021 Apr 16;2021:6611828. doi: 10.1155/2021/6611828. eCollection 2021. Obstet Gynecol Int. 2021. PMID: 33953752 Free PMC article.
-
Maternal and Fetal Outcomes in Preeclampsia: Interrelations Between Insulin Resistance, Aldosterone, Metabolic Syndrome, and Polycystic Ovary Syndrome.J Clin Hypertens (Greenwich). 2015 Oct;17(10):783-5. doi: 10.1111/jch.12613. Epub 2015 Jul 14. J Clin Hypertens (Greenwich). 2015. PMID: 26172964 Free PMC article. No abstract available.
-
Risk factors for adverse maternal and perinatal outcomes in women with preeclampsia: analysis of 1396 cases.J Clin Hypertens (Greenwich). 2018 Jun;20(6):1049-1057. doi: 10.1111/jch.13302. Epub 2018 Apr 30. J Clin Hypertens (Greenwich). 2018. PMID: 29707880 Free PMC article.
-
Effectiveness and safety of 1 vs 4 h blood pressure profile with clinical and laboratory assessment for the exclusion of gestational hypertension and pre-eclampsia: a retrospective study in a university affiliated maternity hospital.BMJ Open. 2015 Nov 18;5(11):e009492. doi: 10.1136/bmjopen-2015-009492. BMJ Open. 2015. PMID: 26582404 Free PMC article.
References
-
- National Collaborating Centre for Women's and Children's Health (UK) . Hypertension in pregnancy: the management of hypertensive disorders during pregnancy. National Institute for Health and Clinical Excellence: Guidance. RCOG Press: London, England; 2010:46. - PubMed
-
- Regitz‐Zagrosek V, BlomstromLundqvist C, Borghi C, et al. ESC Guidelines on the management of cardiovascular diseases during pregnancy: the Task Force on the Management of Cardiovascular Diseases during Pregnancy of the European Society of Cardiology (ESC). Eur Heart J. 2011;32:3147–3197. - PubMed
-
- Khan KS, Wojdyla D, Say L, et al. WHO Analysis of cause of maternal death: a systematic review. Lancet. 2006;367:1066–1074. - PubMed
-
- Chandiramani M, Shennan A. Hypertensive disorders of pregnancy: a UK‐based perspective. Curr Opin Obstet Gynecol. 2008;20:96–101. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
