

Cost-Effectiveness of a Diabetes Pay-For-Performance Program in Diabetes Patients with Multiple Chronic Conditions
- PMID: 26173086
- PMCID: PMC4501765
- DOI: 10.1371/journal.pone.0133163
Cost-Effectiveness of a Diabetes Pay-For-Performance Program in Diabetes Patients with Multiple Chronic Conditions
Abstract
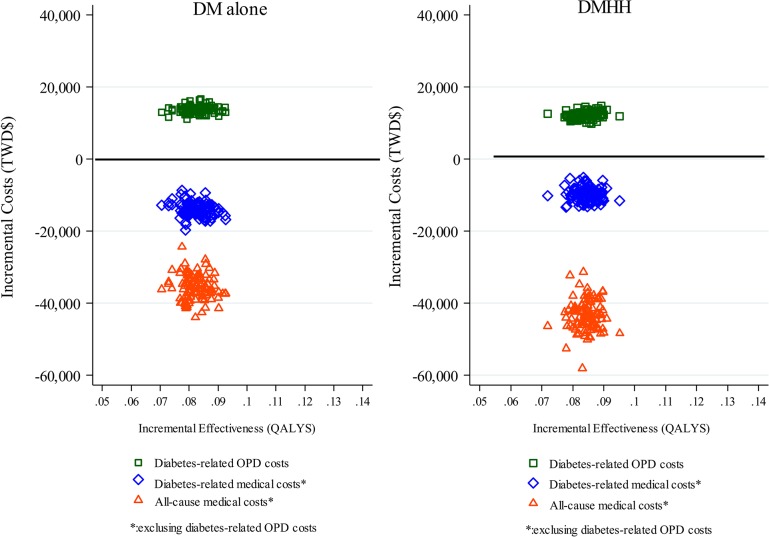
Pay for performance (P4P) has been used as a strategy to improve quality for patients with chronic illness. Little was known whether care provided to individuals with multiple chronic conditions in a P4P program were cost-effective. This study investigated cost effectiveness of a diabetes P4P program for caring patients with diabetes alone (DM alone) and diabetes with comorbid hypertension and hyperlipidemia (DMHH) from a single payer perspective in Taiwan. Analyzing data using population-based longitudinal databases, we compared costs and effectiveness between P4P and non-P4P diabetes patient groups in two cohorts. Propensity score matching (PSM) was used to match comparable control groups for intervention groups. Outcomes included life-years, quality-adjusted life-years (QALYs), program intervention costs, cost-savings and incremental cost-effectiveness ratios (ICERs). QALYs for P4P patients and non-P4P patients were 2.80 and 2.71 for the DM alone cohort and 2.74 and 2.66 for the DMHH patient cohort. The average incremental intervention costs per QALYs was TWD$167,251 in the DM alone cohort and TWD$145,474 in the DMHH cohort. The average incremental all-cause medical costs saved by the P4P program per QALYs were TWD$434,815 in DM alone cohort and TWD$506,199 in the DMHH cohort. The findings indicated that the P4P program for both cohorts were cost-effective and the resulting return on investment (ROI) was 2.60:1 in the DM alone cohort and 3.48:1 in the DMHH cohort. We conclude that the diabetes P4P program in both cohorts enabled the long-term cost-effective use of resources and cost-savings, especially for patients with multiple comorbid conditions.
Conflict of interest statement
Figures
Similar articles
-
Cost-effectiveness of diabetes pay-for-performance incentive designs.Med Care. 2015 Feb;53(2):106-15. doi: 10.1097/MLR.0000000000000264. Med Care. 2015. PMID: 25397966
-
Is a diabetes pay-for-performance program cost-effective under the National Health Insurance in Taiwan?Qual Life Res. 2014 Mar;23(2):687-96. doi: 10.1007/s11136-013-0502-x. Epub 2013 Aug 23. Qual Life Res. 2014. PMID: 23975377
-
Associations between participation in a diabetes pay-for-performance program and health outcomes and healthcare utilization among people with comorbid schizophrenia and type 2 diabetes in Taiwan.Gen Hosp Psychiatry. 2025 May-Jun;94:99-107. doi: 10.1016/j.genhosppsych.2025.02.025. Epub 2025 Mar 2. Gen Hosp Psychiatry. 2025. PMID: 40043624
-
Effects of pay-for-performance for primary care physicians on diabetes outcomes in single-payer health systems: a systematic review.Eur J Health Econ. 2019 Dec;20(9):1303-1315. doi: 10.1007/s10198-019-01097-4. Epub 2019 Aug 10. Eur J Health Econ. 2019. PMID: 31401699
-
Chronic care model in the diabetes pay-for-performance program in Taiwan: Benefits, challenges and future directions.World J Diabetes. 2021 May 15;12(5):578-589. doi: 10.4239/wjd.v12.i5.578. World J Diabetes. 2021. PMID: 33995846 Free PMC article. Review.
Cited by
-
Existing Data Sources in Clinical Epidemiology: The Taiwan National Health Insurance Laboratory Databases.Clin Epidemiol. 2021 Mar 1;13:175-181. doi: 10.2147/CLEP.S286572. eCollection 2021. Clin Epidemiol. 2021. PMID: 33688263 Free PMC article. Review.
-
The Impact of Payment Reforms on the Quality and Utilisation of Healthcare for Patients With Multimorbidity: A Systematic Review.Int J Integr Care. 2022 Feb 10;22(1):10. doi: 10.5334/ijic.5937. eCollection 2022 Jan-Mar. Int J Integr Care. 2022. PMID: 35221826 Free PMC article.
-
Gendered effects of pay for performance among family physicians for chronic disease care: an economic evaluation in a context of universal health coverage.Hum Resour Health. 2019 May 31;17(1):40. doi: 10.1186/s12960-019-0378-0. Hum Resour Health. 2019. PMID: 31151400 Free PMC article.
-
Effectiveness of Nationwide COPD Pay-for-Performance Program on COPD Exacerbations in Taiwan.Int J Chron Obstruct Pulmon Dis. 2021 Oct 18;16:2869-2881. doi: 10.2147/COPD.S329454. eCollection 2021. Int J Chron Obstruct Pulmon Dis. 2021. PMID: 34703221 Free PMC article.
-
Assessing Taiwan's pay-for-performance program for diabetes care: a cost-benefit net value approach.Eur J Health Econ. 2023 Jul;24(5):717-733. doi: 10.1007/s10198-022-01504-3. Epub 2022 Aug 22. Eur J Health Econ. 2023. PMID: 35995886
References
-
- Boyd CM, Fortin M. Future of Multimorbidity Research: How Should Understanding of Multimorbidity Inform Health System Design? Public Health Reviews. 2010;32(2):451–74.
-
- Piette JD, Kerr EA. The impact of comorbid chronic conditions on diabetes care. Diabetes Care. 2006;29(3):725–31. . - PubMed
-
- Wolff JL, Starfield B, Anderson G. Prevalence, expenditures, and complications of multiple chronic conditions in the elderly. Arch Intern Med. 2002;162(20):2269–76. . - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
