

Interrogation of esophagogastric junction barrier function using the esophagogastric junction contractile integral: an observational cohort study
- PMID: 26173375
- PMCID: PMC4757502
- DOI: 10.1111/dote.12389
Interrogation of esophagogastric junction barrier function using the esophagogastric junction contractile integral: an observational cohort study
Abstract
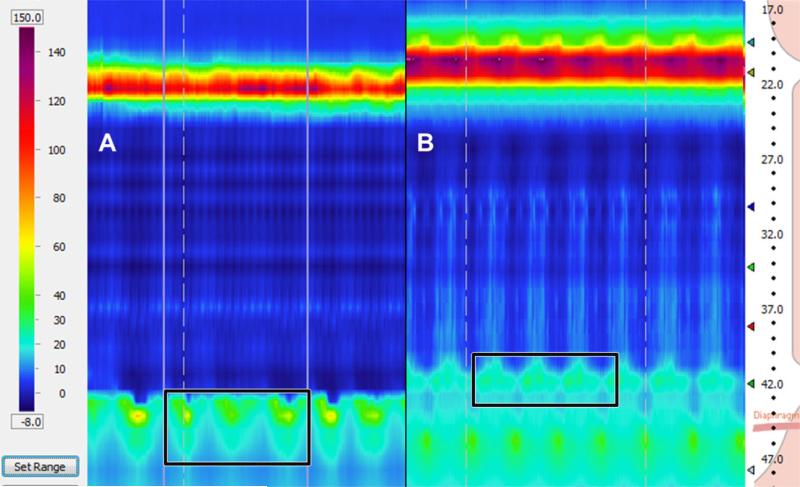
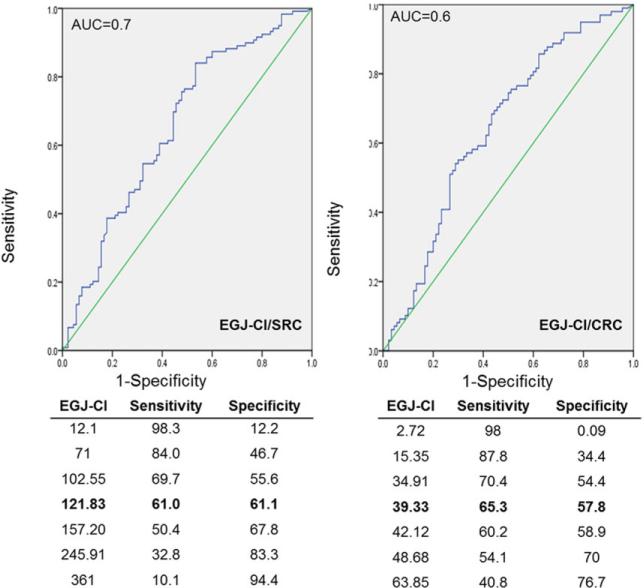
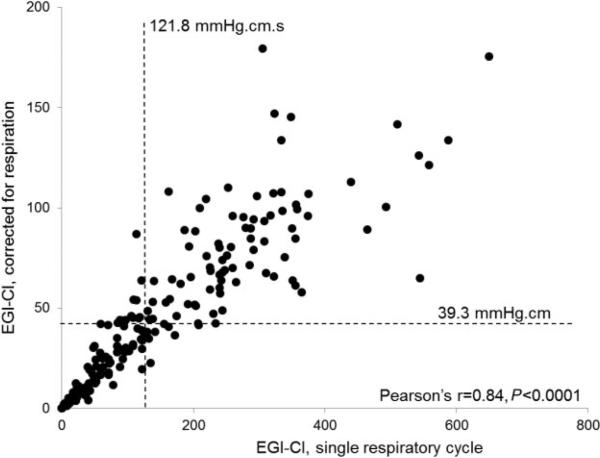
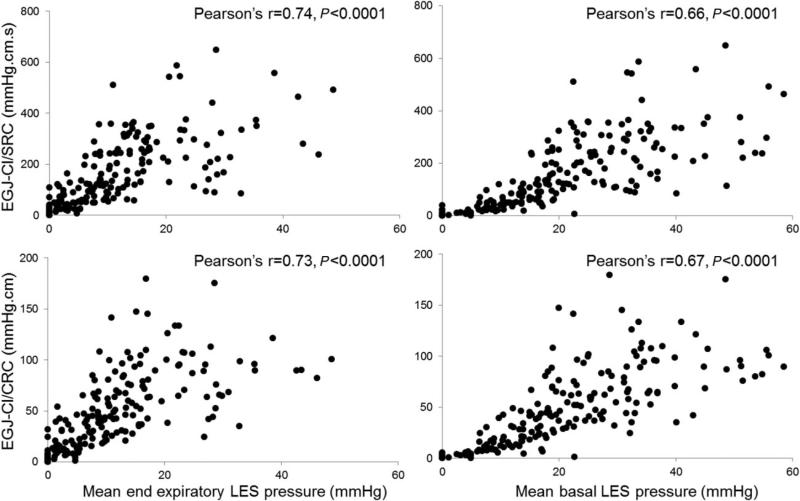
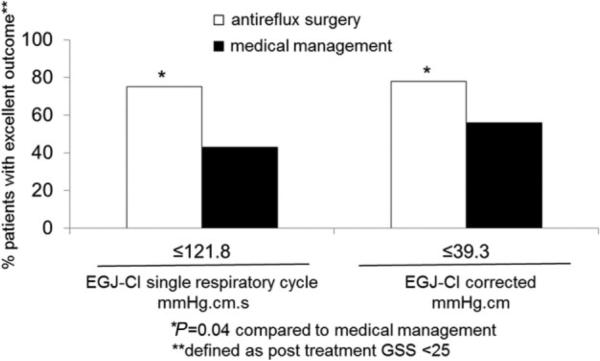
The esophagogastric junction contractile integral (EGJ-CI), designed similar to distal contractile integral (DCI), has been proposed as a metric to evaluate EGJ barrier function. We determined normative values and evaluated EGJ-CI in predicting esophageal acid exposure time (AET) and symptomatic outcome in this observational cohort study. High-resolution manometry (HRM) studies were reviewed in 188 patients (55.2 ± 0.9 years, 64% female) undergoing ambulatory pH monitoring off therapy. Dominant symptoms and global symptom severity (GSS) were determined on questionnaires initially and upon follow-up. EGJ-CI was measured using the DCI tool placed across the EGJ and compared to normal controls (n = 21, 27.6 ± 0.6 years, 52% female). EGJ-CI was calculated both for a single respiratory cycle (SRC, in mmHg.cm.s) and corrected for respiratory cycle (CRC, mmHg.cm). Univariate and multivariate analyses determined the predictive potential of EGJ-CI in terms of AET and post-therapy GSS at follow-up, controlling for medical versus surgical therapy. Mean EGJ-CI values were significantly lower when AET was abnormal; EGJ-CI/SRC and EGJ-CI/CRC were 86% concordant (r = 0.84). Using receiver operating characteristic analysis, values below 121.8 mmHg.cm.s (EGJ-CI/SRC) and 39.3 mmHg.cm (EGJ-CI/CRC) predicted abnormal AET best (sensitivity 0.61 and 0.65, specificity 0.61 and 0.57, respectively). On univariate and multivariate analysis, the EGJ-CI discriminated normal from abnormal AET better than conventional LES parameters (P ≤ 0.02). After 2.7 ± 0.1 years follow-up, EGJ-CI below identified thresholds predicted better symptom response to antireflux surgery compared to medical therapy (P = 0.009). EGJ-CI is a novel HRM metric that has potential to complement or replace currently used basal LES and EGJ parameters.
Keywords: esophagogastric junction; gastroesophageal reflux disease; high-resolution manometry.
© 2015 International Society for Diseases of the Esophagus.
Figures
References
-
- Mittal RK, Balaban DH. The esophagogastric junction. N Engl J Med. 1997;336:924–32. - PubMed
-
- Shaker R, Dodds WJ, Kahrilas PJ, et al. Relationship of intraluminal pH and pressure within the lower esophageal sphincter. Am J Gastroenterol. 1991;86:812–6. - PubMed
-
- Bredenoord AJ, Weusten BL, Timmer R, et al. Intermittent spatial separation of diaphragm and lower esophageal sphincter favors acidic and weakly acidic reflux. Gastroenterology. 2006;130:334–40. - PubMed
-
- Sloan S, Kahrilas PJ. Impairment of esophageal emptying with hiatal hernia. Gastroenterology. 1991;100:596–605. - PubMed
-
- Chan WW, Haroian LR, Gyawali CP. Value of preoperative esophageal function studies before laparoscopic antireflux surgery. Surg Endosc. 2011;25:2943–9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
