

Patient Perceptions of Whom is Most Involved in Their Care with Successive Duty Hour Limits
- PMID: 26173513
- PMCID: PMC4539331
- DOI: 10.1007/s11606-015-3239-0
Patient Perceptions of Whom is Most Involved in Their Care with Successive Duty Hour Limits
Abstract
Background: Although direct patient care is necessary for experiential learning during residency, inpatient perceptions of the roles of resident and attending physicians in their care may have changed with residency duty hours.
Objective: We aimed to assess if patients' perceptions of who is most involved in their care changed with residency duty hours.
Design: This was a prospective observational study over 12 years at a single institution.
Participants: Participants were 22,408 inpatients admitted to the general medicine teaching service from 2001 to 2013, who completed a 1-month follow-up phone interview.
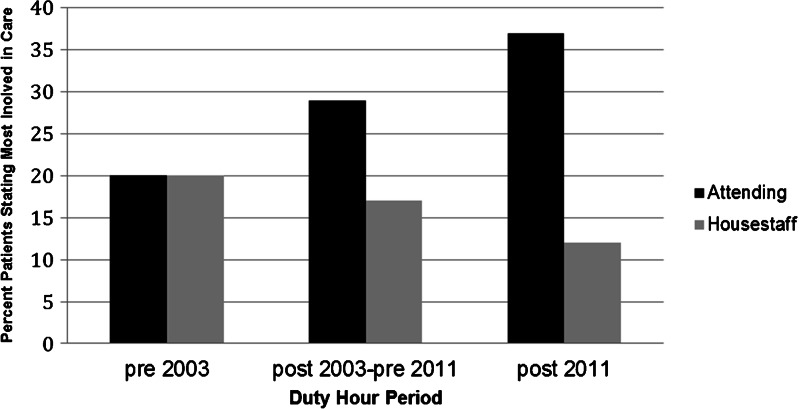
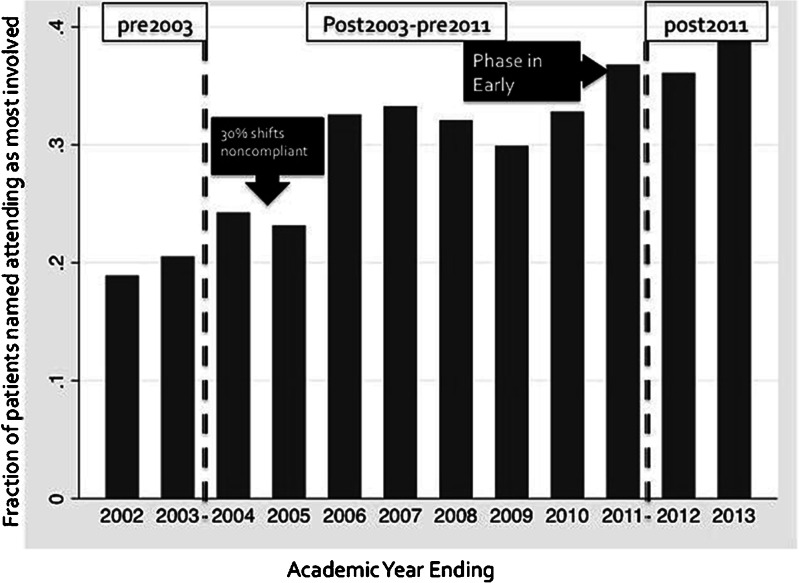
Main measures: Percentage of inpatients who reported an attending, resident, or intern as most involved in their care by duty hour period (pre-2003, post-2003-pre-2011, post-2011).
Key results: With successive duty hour limits, the percentage of patients who reported the attending as most involved in their care increased (pre-2003 20 %, post-2003-pre-2011 29 %, post-2011 37 %, p < 0.001). Simultaneously, fewer patients reported a housestaff physician (resident or intern) as most involved in their care (pre-2003 20 %, post-2003-pre-2011 17 %, post-2011 12 %, p < 0.001). In multinomial regression models controlling for patient age, race, gender and hospitalist as teaching attending, the relative risk ratio of naming the resident versus the attending was higher in the pre-2003 period (1.44, 95 % CI 1.28-1.62, p < 0.001) than the post-2003-pre-2011 (reference group). In contrast, the relative risk ratio for naming the resident versus the attending was lower in the post-2011 period (0.79, 95 % CI 0.68-0.93, p = 0.004) compared to the reference group.
Conclusions: After successive residency duty hours limits, hospitalized patients were more likely to report the attending physician and less likely to report the resident or intern as most involved in their hospital care. Given the importance of experiential learning to the formation of clinical judgment for independent practice, further study on the implications of these trends for resident education and patient safety is warranted.
Figures
Similar articles
-
Resident duty hour modification affects perceptions in medical education, general wellness, and ability to provide patient care.BMC Med Educ. 2016 Jul 13;16:175. doi: 10.1186/s12909-016-0703-4. BMC Med Educ. 2016. PMID: 27411835 Free PMC article.
-
Number of General Medicine Hospital Admissions Performed by Internal Medicine Residents Before and After the 2011 Duty-Hour Regulations.South Med J. 2015 Aug;108(8):476-81. doi: 10.14423/SMJ.0000000000000323. South Med J. 2015. PMID: 26280773
-
Resident perceptions of the impact of duty hour restrictions on resident-attending interactions: an exploratory study.BMC Med Educ. 2017 Jul 18;17(1):124. doi: 10.1186/s12909-017-0963-7. BMC Med Educ. 2017. PMID: 28720087 Free PMC article.
-
Resident duty-hour restrictions-who are we protecting?: AOA critical issues.J Bone Joint Surg Am. 2012 Sep 5;94(17):e131. doi: 10.2106/JBJS.J.01685. J Bone Joint Surg Am. 2012. PMID: 22992860 Review.
-
The declining demand for hospital care as a rationale for duty hour reform.J Gen Intern Med. 2014 Oct;29(10):1400-3. doi: 10.1007/s11606-014-2901-2. Epub 2014 May 28. J Gen Intern Med. 2014. PMID: 24866469 Free PMC article. Review.
Cited by
-
Changes in Patient Perceptions of the Provider Most Involved in Care During COVID-19 and Corresponding Effects on Patient Trust.J Patient Exp. 2023 Apr 3;10:23743735231166501. doi: 10.1177/23743735231166501. eCollection 2023. J Patient Exp. 2023. PMID: 37035096 Free PMC article.
-
The impact of shortening shifts of physicians during their residency on patients and physicians : A systematic review and meta-analysis.Isr J Health Policy Res. 2025 Sep 3;14(1):53. doi: 10.1186/s13584-025-00715-2. Isr J Health Policy Res. 2025. PMID: 40898331 Free PMC article.
-
Hospitalists, value and the future.Future Hosp J. 2016 Feb;3(1):62-64. doi: 10.7861/futurehosp.3-1-62. Future Hosp J. 2016. PMID: 31098182 Free PMC article.
-
Time for System Redesign.J Gen Intern Med. 2015 Sep;30(9):1239-40. doi: 10.1007/s11606-015-3426-z. J Gen Intern Med. 2015. PMID: 26173536 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
