

Avoidability of hospital deaths and association with hospital-wide mortality ratios: retrospective case record review and regression analysis
- PMID: 26174149
- PMCID: PMC4502415
- DOI: 10.1136/bmj.h3239
Avoidability of hospital deaths and association with hospital-wide mortality ratios: retrospective case record review and regression analysis
Abstract
Objectives: To determine the proportion of avoidable deaths (due to acts of omission and commission) in acute hospital trusts in England and to determine the association with the trust's hospital-wide standardised mortality ratio assessed using the two commonly used methods--the hospital standardised mortality ratio (HSMR) and the summary hospital level mortality indicator (SHMI).
Design: Retrospective case record review of deaths.
Setting: 34 English acute hospital trusts (10 in 2009 and 24 in 2012/13) randomly selected from across the spectrum of HSMR.
Main outcome measures: Avoidable death, defined as those with at least a 50% probability of avoidability in view of trained medical reviewers. Association of avoidable death proportion with the HSMR and the SHMI assessed using regression coefficients, to estimate the increase in avoidable death proportion for a one standard deviation increase in standardised mortality ratio.
Participants: 100 randomly selected hospital deaths from each trust.
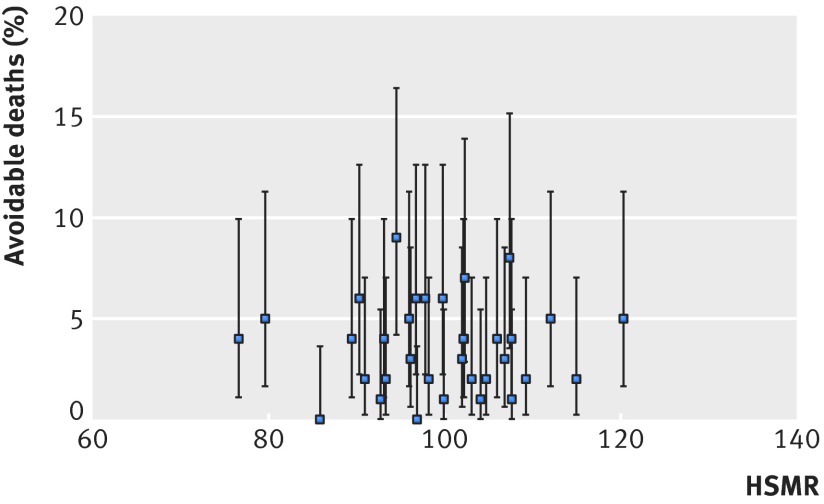
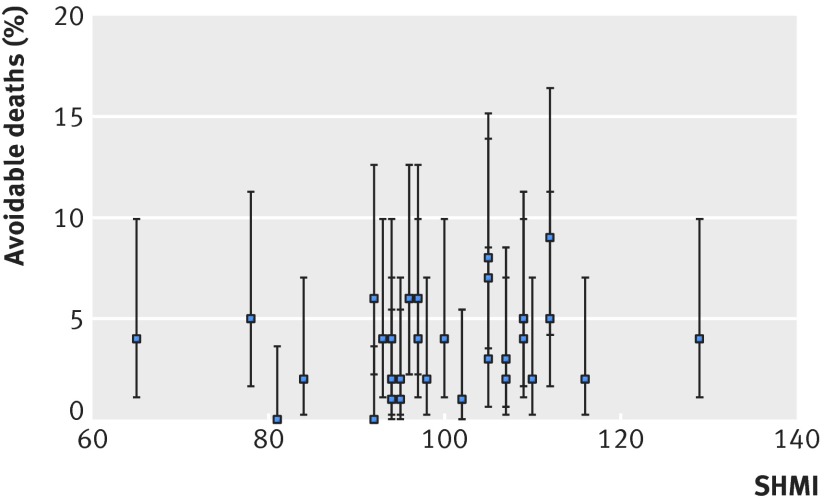
Results: The proportion of avoidable deaths was 3.6% (95% confidence interval 3.0% to 4.3%). It was lower in 2012/13 (3.0%, 2.4% to 3.7%) than in 2009 (5.2%, 3.8% to 6.6%). This difference is subject to several factors, including reviewers' greater awareness in 2012/13 of orders not to resuscitate, patients being perceived as sicker on admission, minor differences in review form questions, and cultural changes that might have discouraged reviewers from criticising other clinicians. There was a small but statistically non-significant association between HSMR and the proportion of avoidable deaths (regression coefficient 0.3, 95% confidence interval -0.2 to 0.7). The regression coefficient was similar for both time periods (0.1 and 0.3). This implies that a difference in HSMR of between 105 and 115 would be associated with an increase of only 0.3% (95% confidence interval -0.2% to 0.7%) in the proportion of avoidable deaths. A similar weak non-significant association was observed for SHMI (regression coefficient 0.3, 95% confidence interval -0.3 to 1.0).
Conclusions: The small proportion of deaths judged to be avoidable means that any metric based on mortality is unlikely to reflect the quality of a hospital. The lack of association between the proportion of avoidable deaths and hospital-wide SMRs partly reflects methodological shortcomings in both metrics. Instead, reviews of individual deaths should focus on identifying ways of improving the quality of care, whereas the use of standardised mortality ratios should be restricted to assessing the quality of care for conditions with high case fatality for which good quality clinical data exist.
© Hogan et al 2015.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
Comment in
-
The death of death rates?BMJ. 2015 Jul 14;351:h3466. doi: 10.1136/bmj.h3466. BMJ. 2015. PMID: 26174623 No abstract available.
-
Standardised mortality ratios should not be used to benchmark hospitals, study concludes.BMJ. 2015 Jul 14;351:h3829. doi: 10.1136/bmj.h3829. BMJ. 2015. PMID: 26179297 No abstract available.
References
-
- Peterson ED, Roe MT, Mulgund J, et al. Association between hospital process performance and outcomes among patients with acute coronary syndromes. JAMA 2006;295:1912-20. - PubMed
-
- Jha AK, Orav EJ, Li Z, et al. The inverse relationship between mortality rates and performance in the Hospital Quality Alliance measures. Health Aff 2007;26:1104-10. - PubMed
-
- Brooke BS, Perler BA, Dominici F, et al. Reduction of in-hospital mortality among California hospitals meeting Leapfrog evidence-based standards for abdominal aortic aneurysm repair. J Vasc Surg 2008;47:1155-64. - PubMed
-
- Shahian DM, Meyer GS, Mort E, et al. Association of National Hospital Quality Measure adherence with long-term mortality and readmissions. BMJ Qual Saf 2012;21:325-36. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical