

Prediction of outcomes by early treatment responses in childhood T-cell acute lymphoblastic leukemia: a retrospective study in China
- PMID: 26174476
- PMCID: PMC4502910
- DOI: 10.1186/s12887-015-0390-z
Prediction of outcomes by early treatment responses in childhood T-cell acute lymphoblastic leukemia: a retrospective study in China
Abstract
Background: Early treatment responses are important prognostic factors in childhood T-cell acute lymphoblastic leukemia (T-ALL) patients. The predictive values of early treatment responses in Chinese childhood T-ALL patients were still unknown.
Methods: From January 2003 to December 2012, 74 consecutive patients aged ≤ 15 years with newly diagnosed T-ALL were treated with BCH-2003 protocol or CCLG-2008 protocol in the Department of Pediatric, Institute of Hematology and Blood Diseases Hospital in China. Predictive values of early treatment responses, including prednisone response, bone marrow morphology at day 15 and day 33 during induction chemotherapy, and minimal residual disease (MRD) monitored by flow cytometry after induction therapy (time point 1, TP1) and before consolidation therapy (time point 2, TP2), were analyzed.
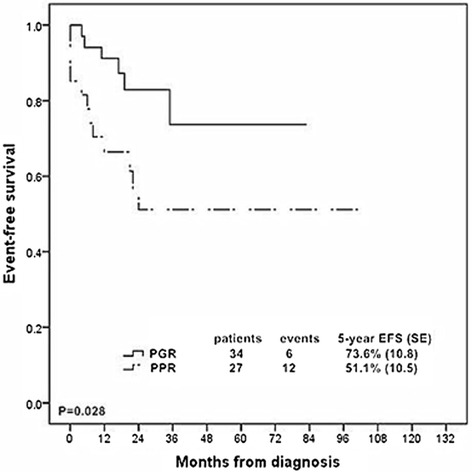
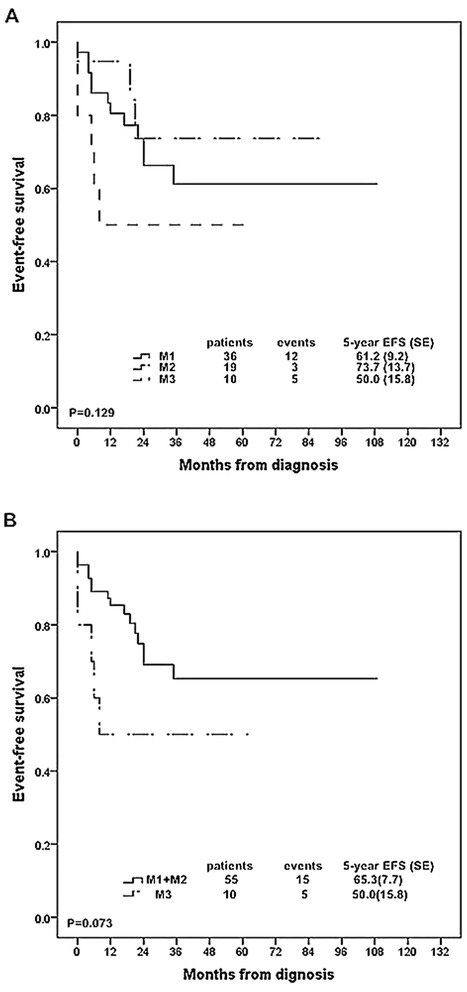
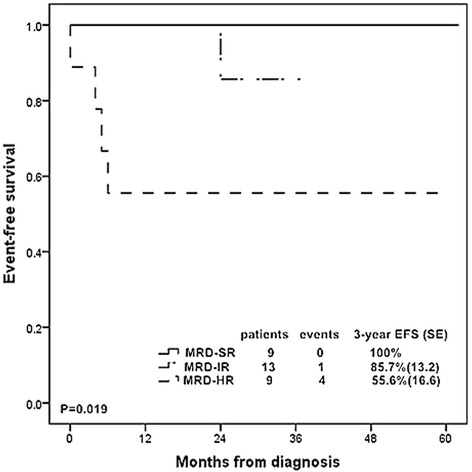
Results: The 5-year event free survival (EFS) and overall survival (OS) rates for these patients were 62.5% (SE, 6.4) and 62.7% (SE, 6.6), respectively. Prednisone poor responder was strongly associated with increased chance of induction failure (14.8%) and decreased survival rate (5 year EFS rate, 51.1 % (SE, 10.5)). Patients with ≥ 25% blast cells in bone marrow at day 15 were more likely to have an inferior outcome. 93.2% of the T-ALL patients achieved complete remission at day 33 while patients with resistant disease all died of disease progression. MRD ≥ 10(-2) at TP1 or MRD ≥ 10(-3) at TP2 was significantly related to dismal prognosis. Risk groups classified by MRD at two time points could stratify patients into different groups: 29.0% of the patients were MRD standard risk (MRD < 10(-4) at both time points) with 3-year EFS rate of 100%, 29.0% were MRD high risk (MRD ≥ 10(-2) at TP1 or MRD ≥ 10(-2) at TP2) with 3-year EFS rate of 55.6% (SE, 16.6) , and the rest of patients were defined as MRD intermediate risk with 3-year EFS rate of 85.7% (SE, 13.2).
Conclusion: Our study demonstrated that MRD was the most powerful predictor of treatment outcome in childhood T-ALL patients and conventional morphological assessments of treatment response still played important roles in predicting treatment outcome and tailoring treatment intensity especially in countries with inadequate skills or financial resources for MRD monitoring.
Figures

References
-
- Uckun FM, Sensel MG, Sun L, Steinherz PG, Trigg ME, Heerema NA, Sather HN, Reaman GH, Gaynon PS. Biology and treatment of childhood T-lineage acute lymphoblastic leukemia. Blood. 1998;91(3):735–746. - PubMed
-
- Goldberg JM, Silverman LB, Levy DE, Dalton VK, Gelber RD, Lehmann L, Cohen HJ, Sallan SE, Asselin BL. Childhood T-cell acute lymphoblastic leukemia: the Dana-Farber Cancer Institute acute lymphoblastic leukemia consortium experience. J Clin Oncol. 2003;21(19):3616–3622. doi: 10.1200/JCO.2003.10.116. - DOI - PubMed
-
- Möricke A, Reiter A, Zimmermann M, Gadner H, Stanulla M, Dördelmann M, Löning L, Beier R, Ludwig WD, Ratei R, Harbott J, Boos J, Mann G, Niggli F, Feldges A, Henze G, Welte K, Beck JD, Klingebiel T, Niemeyer C, Zintl F, Bode U, Urban C, Wehinger H, Niethammer D, Riehm H, Schrappe M, German-Austrian-Swiss ALL-BFM Study Group Risk-adjusted therapy of acute lymphoblastic leukemia can decrease treatment burden and improve survival: treatment results of 2169 unselected pediatric and adolescent patients enrolled in the trial ALL-BFM 95. Blood. 2008;111(9):4477–4489. doi: 10.1182/blood-2007-09-112920. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
