

Cost-Effectiveness of Surveillance for Bloodstream Infections for Sepsis Management in Low-Resource Settings
- PMID: 26175032
- PMCID: PMC4596611
- DOI: 10.4269/ajtmh.15-0083
Cost-Effectiveness of Surveillance for Bloodstream Infections for Sepsis Management in Low-Resource Settings
Abstract
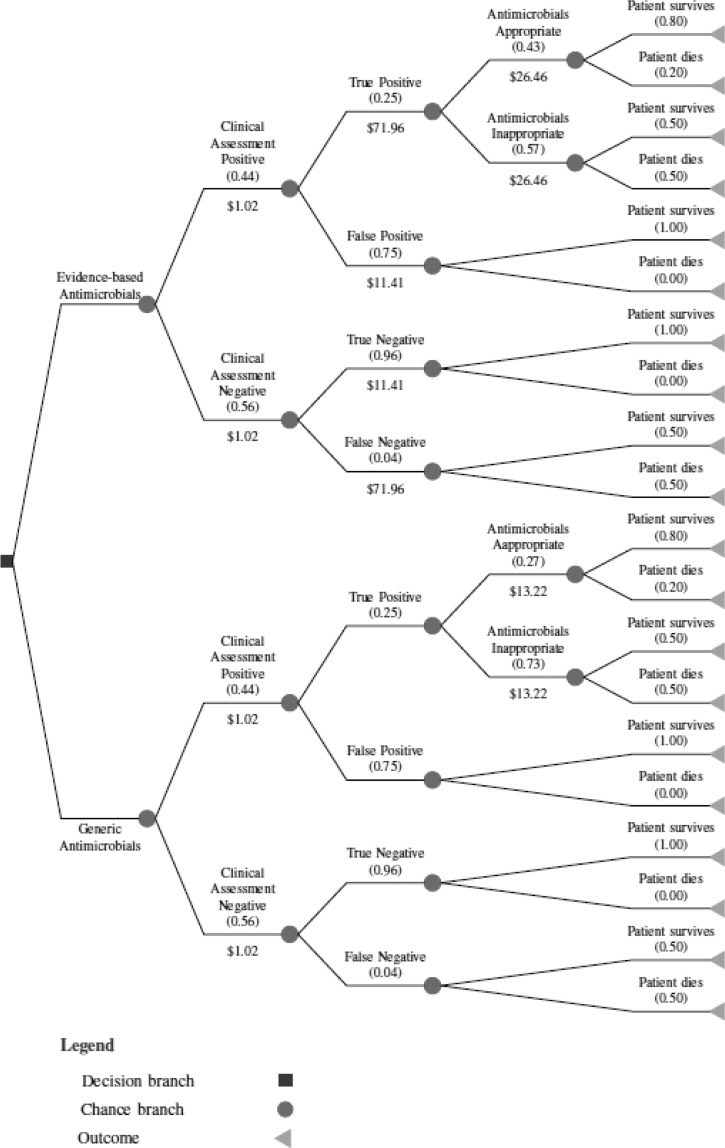
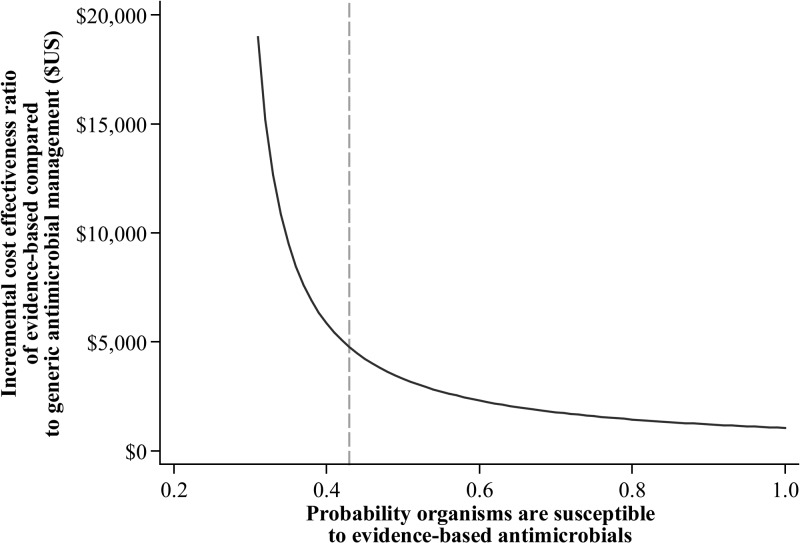
Bacterial sepsis is a leading cause of mortality among febrile patients in low- and middle-income countries, but blood culture services are not widely available. Consequently, empiric antimicrobial management of suspected bloodstream infection is based on generic guidelines that are rarely informed by local data on etiology and patterns of antimicrobial resistance. To evaluate the cost-effectiveness of surveillance for bloodstream infections to inform empiric management of suspected sepsis in low-resource areas, we compared costs and outcomes of generic antimicrobial management with management informed by local data on etiology and patterns of antimicrobial resistance. We applied a decision tree model to a hypothetical population of febrile patients presenting at the district hospital level in Africa. We found that the evidence-based regimen saved 534 more lives per 100,000 patients at an additional cost of $25.35 per patient, resulting in an incremental cost-effectiveness ratio of $4,739. This ratio compares favorably to standard cost-effectiveness thresholds, but should ultimately be compared with other policy-relevant alternatives to determine whether routine surveillance for bloodstream infections is a cost-effective strategy in the African context.
© The American Society of Tropical Medicine and Hygiene.
Figures
References
-
- Deen J, von Seidlein L, Andersen F, Elle N, White NJ, Lubell Y. Community-acquired bacterial bloodstream infections in developing countries in south and southeast Asia: a systematic review. Lancet Infect Dis. 2012;12:480–487. - PubMed
-
- Leibovici L, Shraga I, Drucker M, Konigsberger H, Samra Z, Pitlik SD. The benefit of appropriate empirical antibiotic treatment in patients with bloodstream infection. J Intern Med. 1998;244:379–386. - PubMed
-
- Petti CA, Polage CR, Quinn TC, Ronald AR, Sande MA. Laboratory medicine in Africa: a barrier to effective health care. Clin Infect Dis. 2006;42:377–382. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- R01 TW009237/TW/FIC NIH HHS/United States
- BB/L018845/1/BB_/Biotechnology and Biological Sciences Research Council/United Kingdom
- BB/L017679/BB_/Biotechnology and Biological Sciences Research Council/United Kingdom
- BB/L018845/BB_/Biotechnology and Biological Sciences Research Council/United Kingdom
- BB/J010367/1/BB_/Biotechnology and Biological Sciences Research Council/United Kingdom
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
