

Diagnosis of Gastroesophageal Reflux Disease Using Real-time Magnetic Resonance Imaging
- PMID: 26175205
- PMCID: PMC4648433
- DOI: 10.1038/srep12112
Diagnosis of Gastroesophageal Reflux Disease Using Real-time Magnetic Resonance Imaging
Abstract
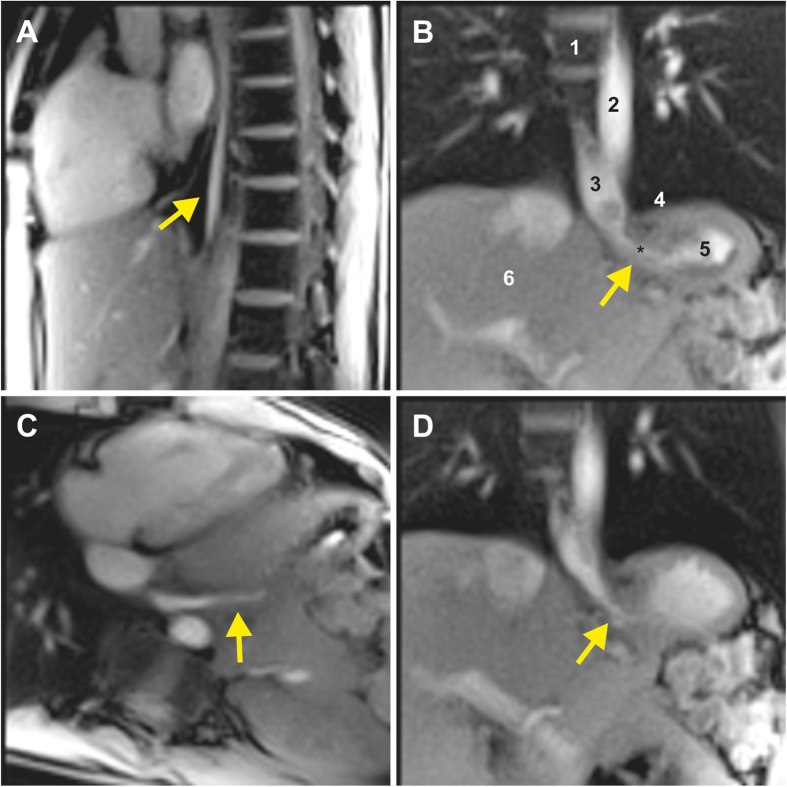
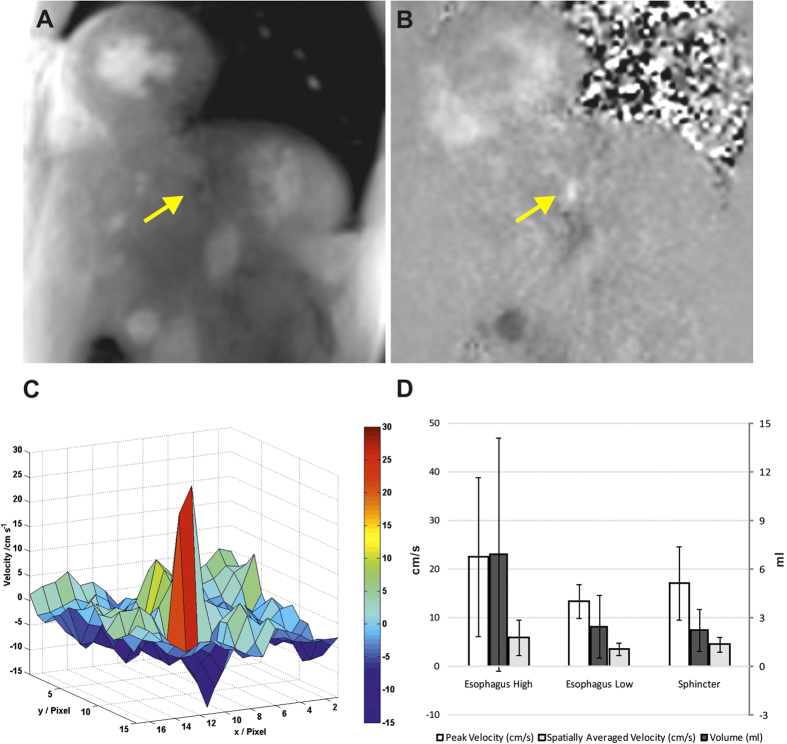
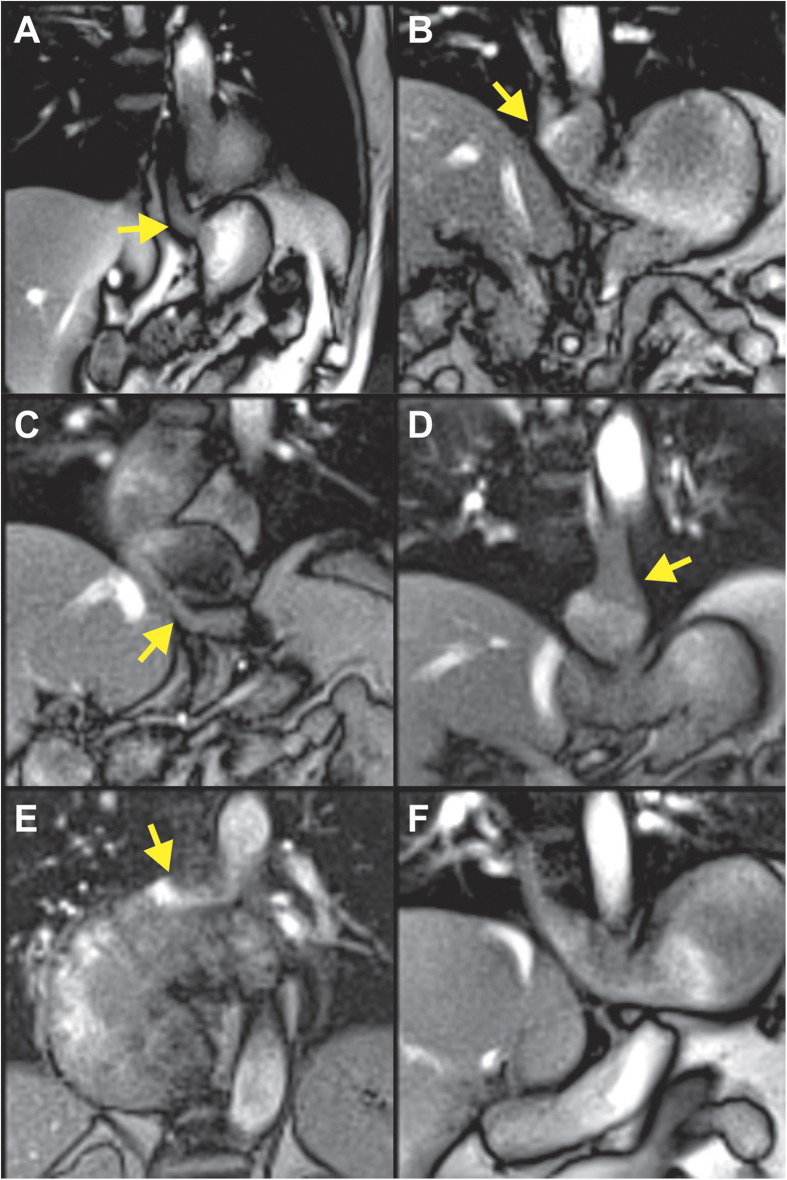
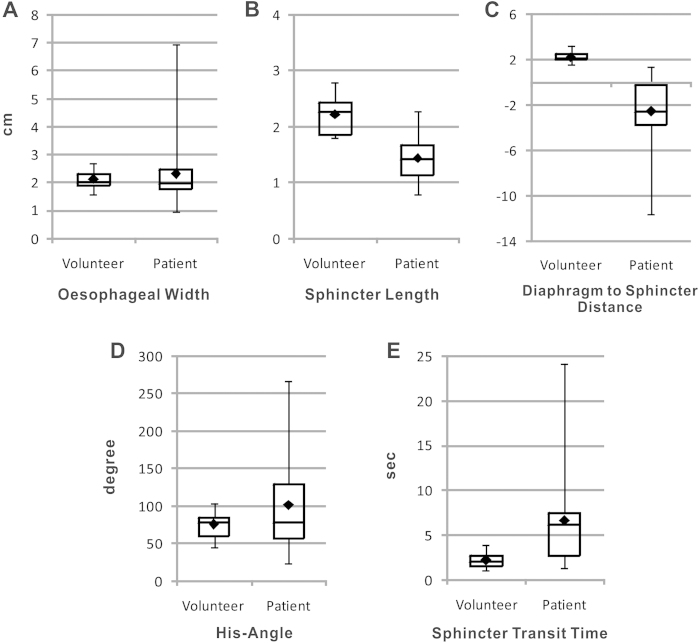
A small angle (His angle) between the oesophagus and the fundus of the stomach is considered to act as flap valve and anti-reflux barrier. A wide angle results in dysfunction of the oesophagogastric junction and subsequently in gastroesophageal reflux disease (GERD). Here, we used real-time magnetic resonance imaging (MRI) at 50 ms resolution (20 frames per second) in 12 volunteers and 12 patients with GERD to assess transport of pineapple juice through the oesophagogastric junction and reflux during Valsalva. We found that the intra-abdominal part of the oesophagus was bended towards the left side resulting in an angle of 75.3 ± 17.4, which was significantly larger during Valsava (P = 0.017). Reflux and several underlying pathologies were detected in 11 out of 12 patients. Our data visualize oesophagogastric junction physiology and disprove the flap valve hypothesis. Further, non-invasive real-time MRI has considerable potential for the diagnosis of causative pathologies leading to GERD.
Conflict of interest statement
S.Z. and J.F. hold a patent on the image acquisition and reconstruction technique used here. None of the other authors have conflicts of interest to declare.
Figures
References
-
- Orr W. C. Review article: sleep-related gastro-oesophageal reflux as a distinct clinical entity. Aliment Pharmacol Ther 31, 47–56 (2010). - PubMed
-
- Galmiche J. P. et al. Functional esophageal disorders. Gastroenterology 130, 1459–1465 (2006). - PubMed
-
- Hill L. D. et al. The gastroesophageal flap valve: in vitro and in vivo observations. Gastrointest Endosc 44, 541–547 (1996). - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
