

Cellular and molecular mechanisms of repair in acute and chronic wound healing
- PMID: 26175283
- PMCID: PMC4671308
- DOI: 10.1111/bjd.13954
Cellular and molecular mechanisms of repair in acute and chronic wound healing
Abstract
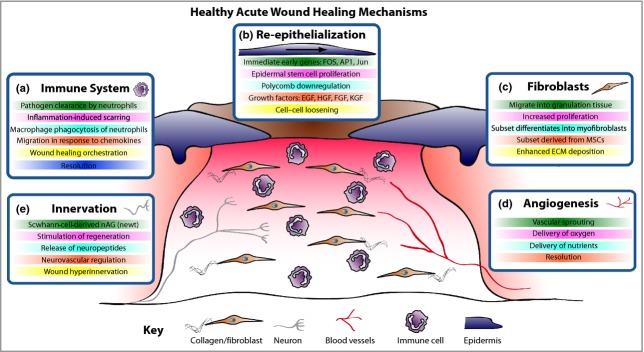
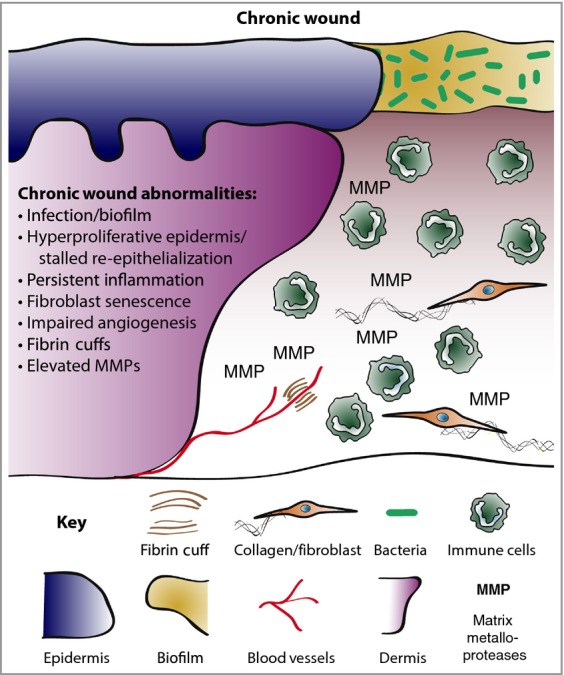
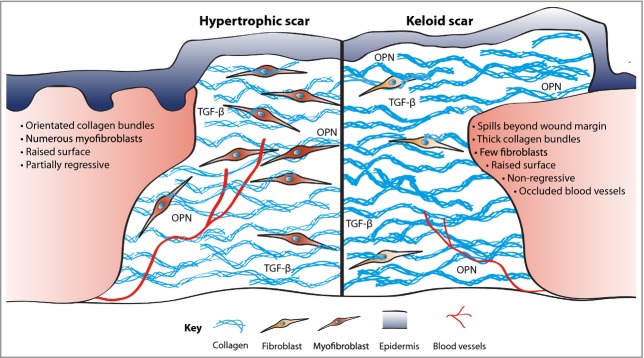
A considerable understanding of the fundamental cellular and molecular mechanisms underpinning healthy acute wound healing has been gleaned from studying various animal models, and we are now unravelling the mechanisms that lead to chronic wounds and pathological healing including fibrosis. A small cut will normally heal in days through tight orchestration of cell migration and appropriate levels of inflammation, innervation and angiogenesis. Major surgeries may take several weeks to heal and leave behind a noticeable scar. At the extreme end, chronic wounds - defined as a barrier defect that has not healed in 3 months - have become a major therapeutic challenge throughout the Western world and will only increase as our populations advance in age, and with the increasing incidence of diabetes, obesity and vascular disorders. Here we describe the clinical problems and how, through better dialogue between basic researchers and clinicians, we may extend our current knowledge to enable the development of novel potential therapeutic treatments.
© 2015 British Association of Dermatologists.
Figures
References
-
- Schultz GS, White M, Mitchell R, et al. Epithelial wound healing enhanced by transforming growth factor-alpha and vaccinia growth factor. Science. 1987;235:350–2. - PubMed
-
- Grose R, Werner S. Wound-healing studies in transgenic and knockout mice. Mol Biotechnol. 2004;28:147–66. - PubMed
-
- Pedersen TX, Leethanakul C, Patel V, et al. Laser capture microdissection-based in vivo genomic profiling of wound keratinocytes identifies similarities and differences to squamous cell carcinoma. Oncogene. 2003;22:3964–76. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
