

Comparison of Ultrasonographic Findings of Biopsy-Proven Tuberculous Lymphadenitis and Kikuchi Disease
- PMID: 26175575
- PMCID: PMC4499540
- DOI: 10.3348/kjr.2015.16.4.767
Comparison of Ultrasonographic Findings of Biopsy-Proven Tuberculous Lymphadenitis and Kikuchi Disease
Abstract
Objective: Although tuberculous lymphadenitis and Kikuchi disease are common causes of cervical lymphadenopathy in Asians and exhibit similar clinical manifestations, their treatment strategies are totally different. The purpose of this study was to identify ultrasonographic features that distinguish these two diseases.
Materials and methods: This study was approved by the Institutional Review Board. The study included 77 patients with tuberculous lymphadenitis and 135 patients with Kikuchi disease. The sex and age distributions of the patients were analyzed. The size and shape of lymph nodes (LNs), presence of conglomeration, increased perinodal echogenicity, echogenic hilum, posterior neck involvement, internal calcification, patterns of internal necrosis, laterality of involved LNs, and hilar vascular patterns on ultrasonography were compared between the two groups. Multiple logistic regression analysis was conducted to identify independent findings to discriminate tuberculous lymphadenitis from Kikuchi disease. Finally, diagnostic accuracies were calculated using the independent findings.
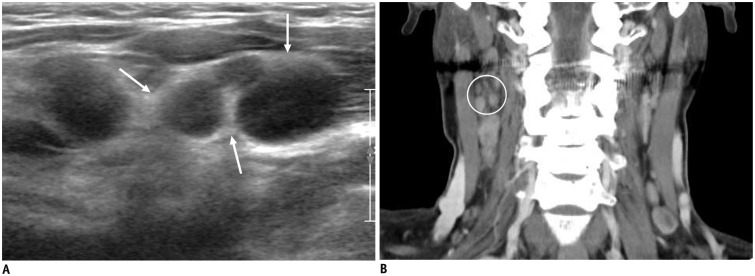
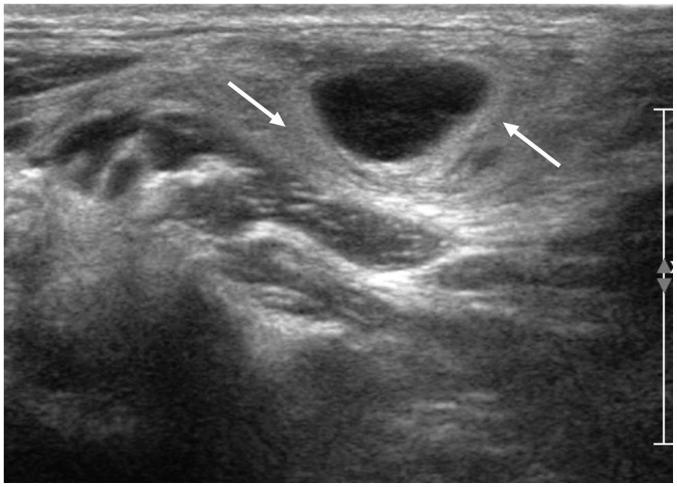
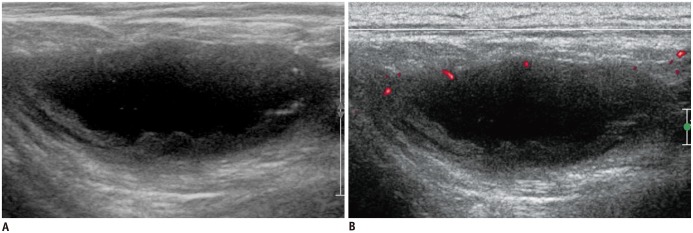
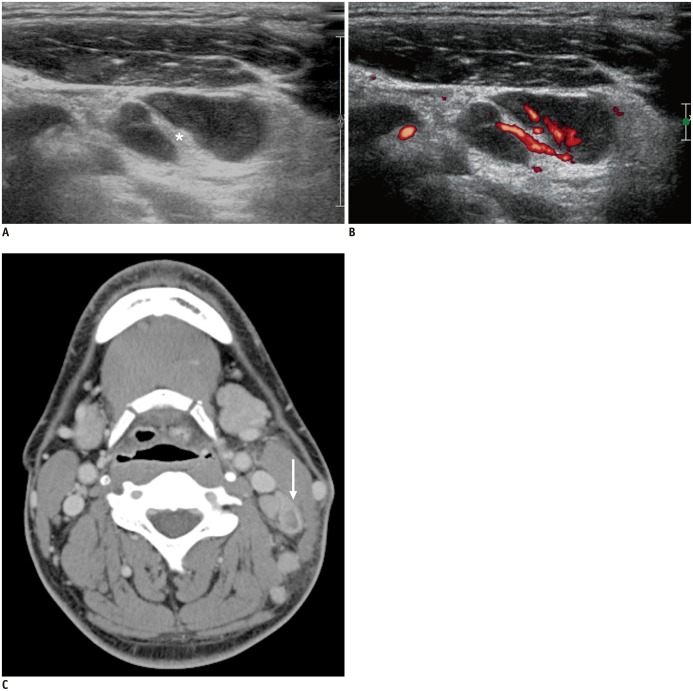
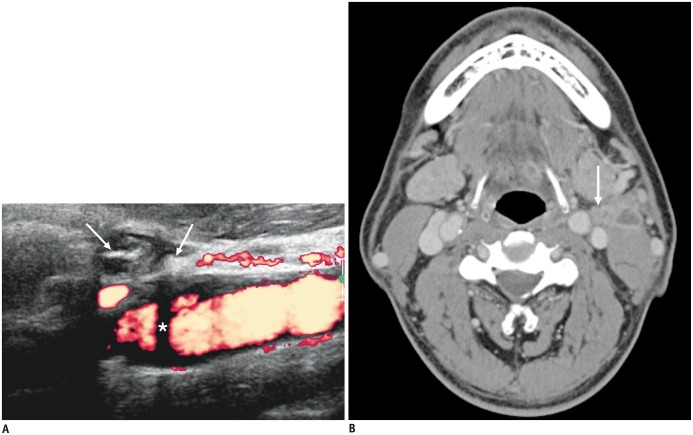
Results: The presence of an echogenic hilum, internal calcification, patterns of internal necrosis, and LN hilar vascular structures on power Doppler ultrasonography were independent findings that discriminated tuberculous lymphadenitis from Kikuchi disease. The diagnostic accuracy of each of these four factors was 84.9% (181/212), 76.9% (163/212), 84% (178/212), and 89.2% (189/212), respectively. A combination of internal calcification and hilar vascular structures showed the best accuracy of 89.6% (190/212) (sensitivity, 86.7% [117/135]; specificity, 94.8% [73/77]) for diagnosing Kikuchi disease.
Conclusion: The presence of an echogenic hilum, internal calcification, pattern of internal necrosis, and LN hilar vascular structures are useful ultrasonographic findings to differentiate tuberculous lymphadenitis from Kikuchi disease.
Keywords: Kikuchi disease; Tuberculosis; Tuberculous lymphadenitis; Ultrasonography.
Figures
Similar articles
-
Cervical lymphadenopathy in children: a diagnostic tree analysis model based on ultrasonographic and clinical findings.Eur Radiol. 2020 Aug;30(8):4475-4485. doi: 10.1007/s00330-020-06794-w. Epub 2020 Mar 18. Eur Radiol. 2020. PMID: 32189052
-
Kikuchi Cervical Lymphadenitis in Children: Ultrasound Differentiation From Common Infectious Lymphadenitis.J Ultrasound Med. 2021 Oct;40(10):2069-2078. doi: 10.1002/jum.15584. Epub 2020 Dec 2. J Ultrasound Med. 2021. PMID: 33263358
-
Gray scale and power Doppler study of biopsy-proven Kikuchi disease.J Ultrasound Med. 2011 Jul;30(7):957-63. doi: 10.7863/jum.2011.30.7.957. J Ultrasound Med. 2011. PMID: 21705728
-
CT pattern analysis of necrotizing and nonnecrotizing lymph nodes in Kikuchi disease.PLoS One. 2017 Jul 24;12(7):e0181169. doi: 10.1371/journal.pone.0181169. eCollection 2017. PLoS One. 2017. PMID: 28742156 Free PMC article.
-
Sonography of neck lymph nodes. Part II: abnormal lymph nodes.Clin Radiol. 2003 May;58(5):359-66. doi: 10.1016/s0009-9260(02)00585-8. Clin Radiol. 2003. PMID: 12727163 Review.
Cited by
-
Acoustic radiation force impulse imaging of biopsy-proven Kikuchi disease: initial experiences for evaluating feasibility in pediatric patients.Ultrasonography. 2019 Jan;38(1):58-66. doi: 10.14366/usg.17067. Epub 2018 Apr 24. Ultrasonography. 2019. PMID: 29914233 Free PMC article.
-
Does the Reporting Quality of Diagnostic Test Accuracy Studies, as Defined by STARD 2015, Affect Citation?Korean J Radiol. 2016 Sep-Oct;17(5):706-14. doi: 10.3348/kjr.2016.17.5.706. Epub 2016 Aug 23. Korean J Radiol. 2016. PMID: 27587959 Free PMC article.
-
Initial experience of a deep learning application for the differentiation of Kikuchi-Fujimoto's disease from tuberculous lymphadenitis on neck CECT.Sci Rep. 2022 Aug 19;12(1):14184. doi: 10.1038/s41598-022-18535-8. Sci Rep. 2022. PMID: 35986073 Free PMC article.
-
Cervical lymphadenopathy in children: a diagnostic tree analysis model based on ultrasonographic and clinical findings.Eur Radiol. 2020 Aug;30(8):4475-4485. doi: 10.1007/s00330-020-06794-w. Epub 2020 Mar 18. Eur Radiol. 2020. PMID: 32189052
-
A Case of Kikuchi-Fujimoto Disease in a 7-Year-Old African American Patient: A Case Report and Review of Literature.Am J Case Rep. 2020 Aug 24;21:e922784. doi: 10.12659/AJCR.922784. Am J Case Rep. 2020. PMID: 32830793 Free PMC article. Review.
References
-
- Onciu M, Medeiros LJ. Kikuchi-Fujimoto lymphadenitis. Adv Anat Pathol. 2003;10:204–211. - PubMed
-
- Song JY, Lee J, Park DW, Sohn JW, Suh SI, Kim IS, et al. Clinical outcome and predictive factors of recurrence among patients with Kikuchi's disease. Int J Infect Dis. 2009;13:322–326. - PubMed
-
- Youk JH, Kim EK, Ko KH, Kim MJ. Sonographic features of axillary lymphadenopathy caused by Kikuchi disease. J Ultrasound Med. 2008;27:847–853. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
