

Common Postmortem Computed Tomography Findings Following Atraumatic Death: Differentiation between Normal Postmortem Changes and Pathologic Lesions
- PMID: 26175579
- PMCID: PMC4499544
- DOI: 10.3348/kjr.2015.16.4.798
Common Postmortem Computed Tomography Findings Following Atraumatic Death: Differentiation between Normal Postmortem Changes and Pathologic Lesions
Abstract
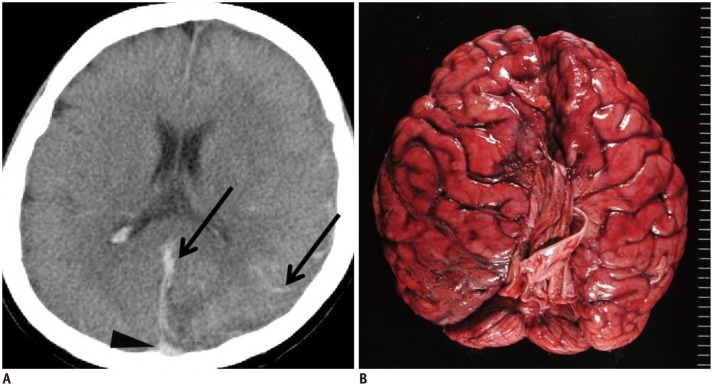
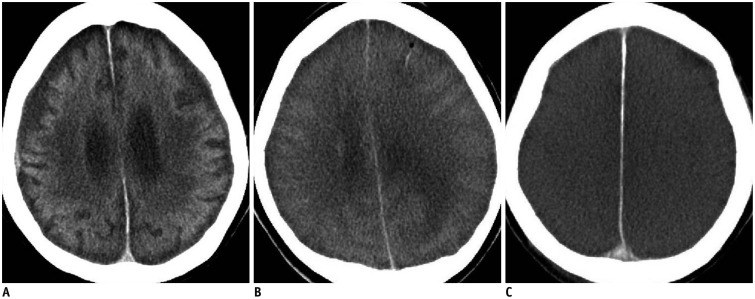
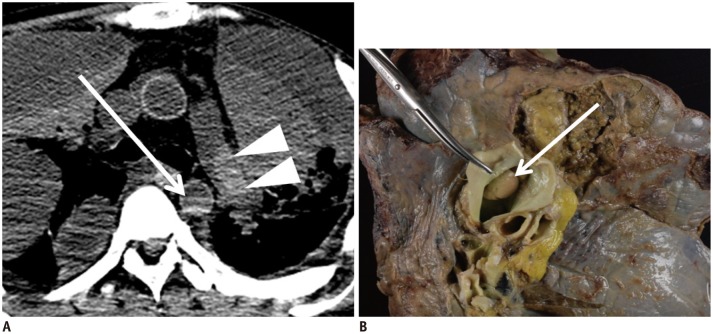
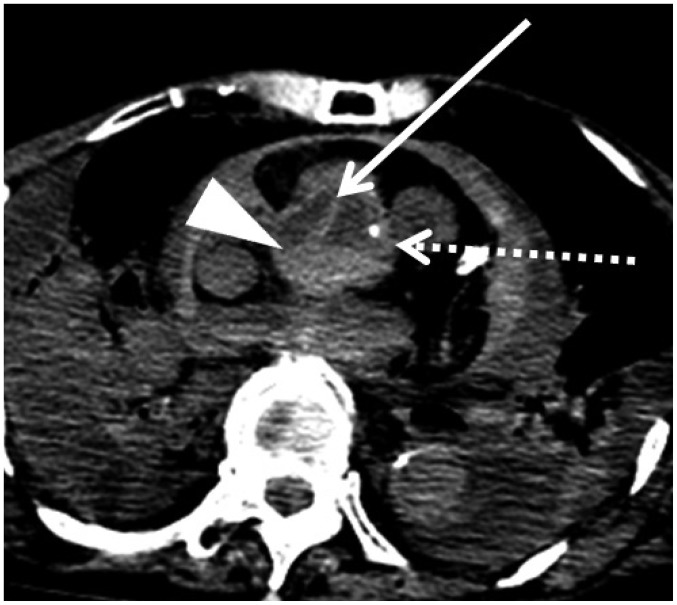
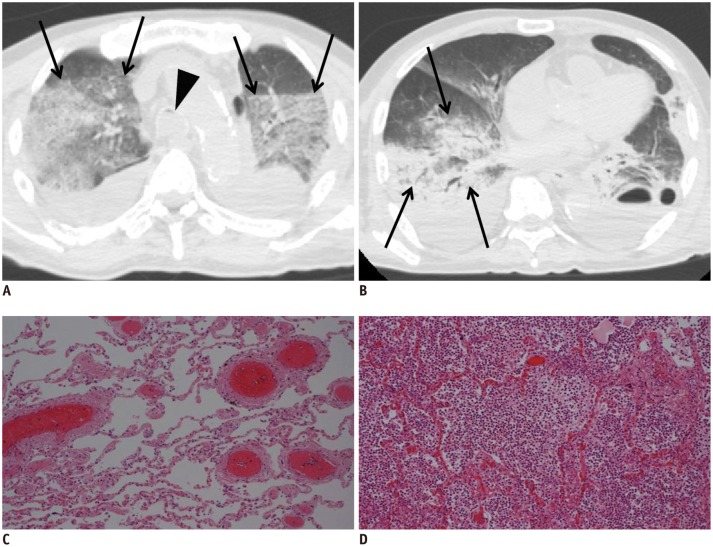
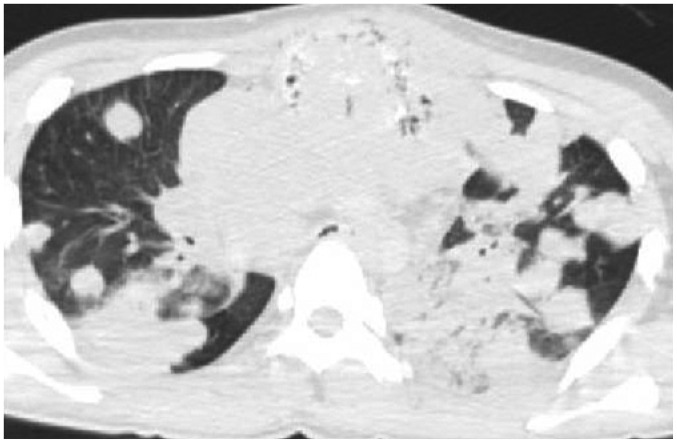
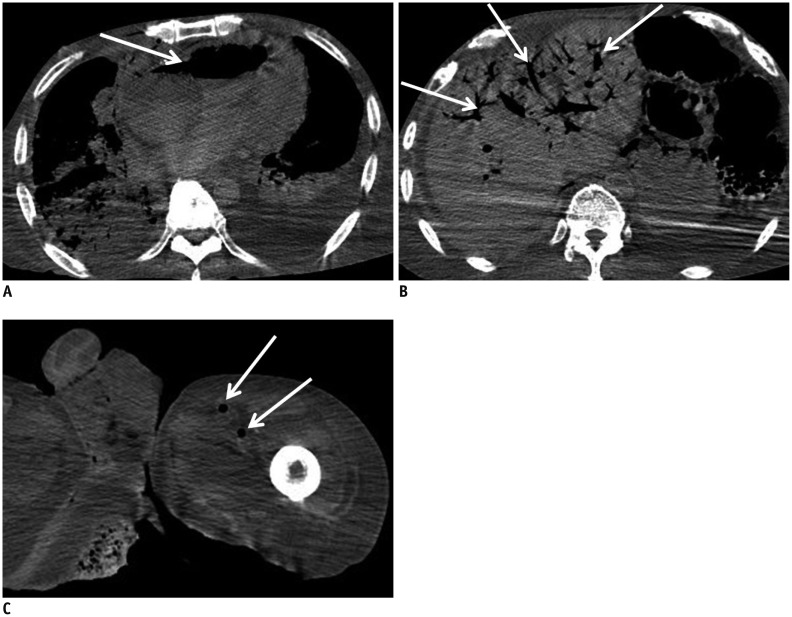
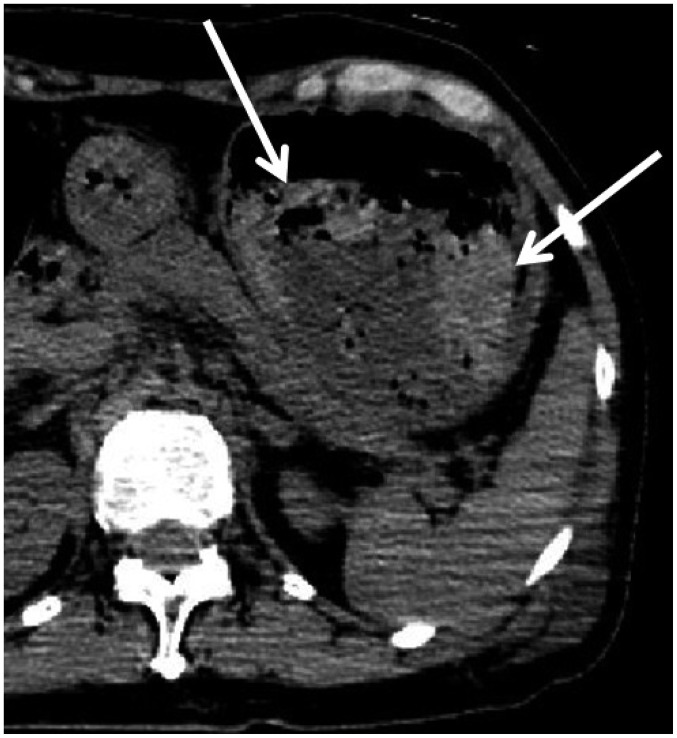
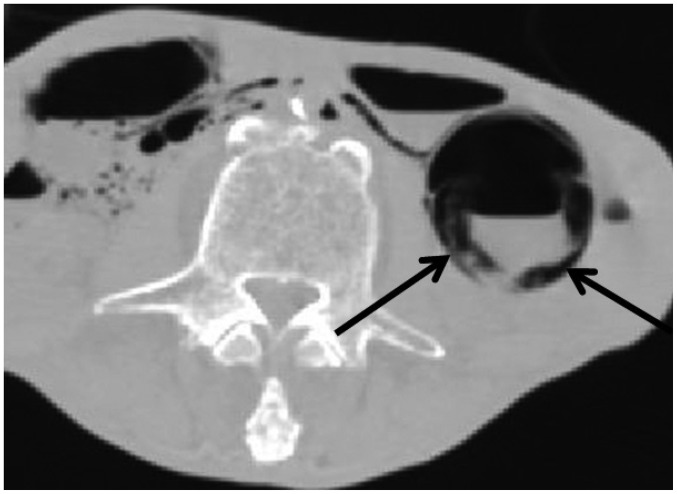
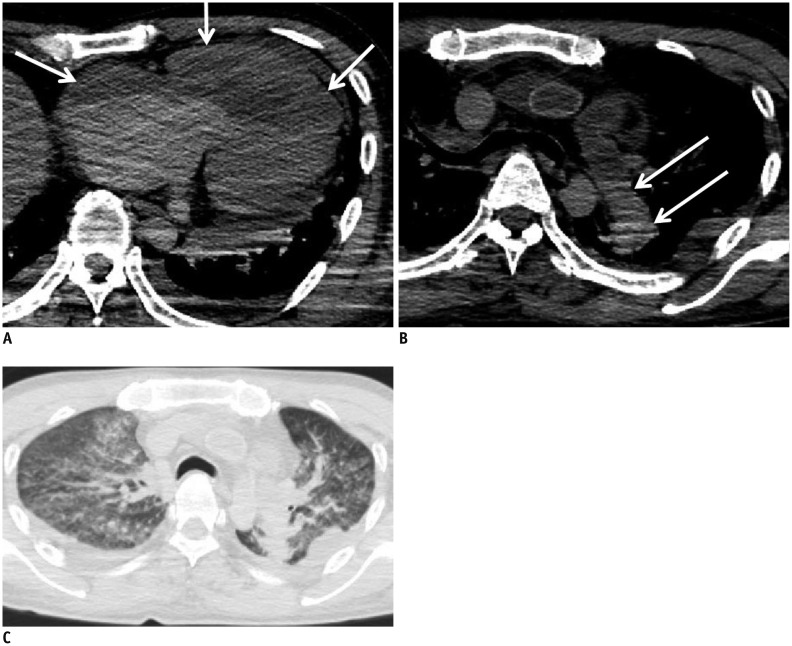
Computed tomography (CT) is widely used in postmortem investigations as an adjunct to the traditional autopsy in forensic medicine. To date, several studies have described postmortem CT findings as being caused by normal postmortem changes. However, on interpretation, postmortem CT findings that are seemingly due to normal postmortem changes initially, may not have been mere postmortem artifacts. In this pictorial essay, we describe the common postmortem CT findings in cases of atraumatic in-hospital death and describe the diagnostic pitfalls of normal postmortem changes that can mimic real pathologic lesions.
Keywords: Autopsy imaging; Forensic radiology; Postmortem CT; Postmortem imaging.
Figures

Similar articles
-
Lung weight estimation with postmortem CT in forensic cases.Leg Med (Tokyo). 2018 Nov;35:61-65. doi: 10.1016/j.legalmed.2018.09.007. Epub 2018 Sep 22. Leg Med (Tokyo). 2018. PMID: 30268692
-
Pediatric postmortem computed tomography: initial experience at a children's hospital in the United States.Pediatr Radiol. 2019 Aug;49(9):1113-1129. doi: 10.1007/s00247-019-04433-1. Epub 2019 Jun 14. Pediatr Radiol. 2019. PMID: 31201439 Review.
-
Postmortem Computed Tomography and Computed Tomography Angiography: Cardiothoracic Imaging Applications in Forensic Medicine.J Thorac Imaging. 2019 Sep;34(5):286-298. doi: 10.1097/RTI.0000000000000398. J Thorac Imaging. 2019. PMID: 30801453 Review.
-
Computer-assisted virtual autopsy using surgical navigation techniques.AJR Am J Roentgenol. 2015 Jan;204(1):W58-62. doi: 10.2214/AJR.13.11957. AJR Am J Roentgenol. 2015. PMID: 25539276
-
Common and expected postmortem CT observations involving the brain: mimics of antemortem pathology.AJNR Am J Neuroradiol. 2012 Aug;33(7):1387-91. doi: 10.3174/ajnr.A2966. Epub 2012 Apr 5. AJNR Am J Neuroradiol. 2012. PMID: 22492568 Free PMC article.
Cited by
-
Significance of intracranial gas on post-mortem computed tomography in traumatic cases in the context of medico-legal opinions.Forensic Sci Med Pathol. 2020 Mar;16(1):3-11. doi: 10.1007/s12024-019-00162-x. Epub 2019 Aug 28. Forensic Sci Med Pathol. 2020. PMID: 31463781 Free PMC article.
-
Postmortem CT scan in intoxication cases: A necessity or just an indulgence.Indian J Radiol Imaging. 2019 Jul-Sep;29(3):305-309. doi: 10.4103/ijri.IJRI_2_19. Epub 2019 Oct 30. Indian J Radiol Imaging. 2019. PMID: 31741600 Free PMC article.
-
Can postmortem computed tomography detect antemortem hypoxic-ischemic encephalopathy?Forensic Sci Med Pathol. 2016 Sep;12(3):267-75. doi: 10.1007/s12024-016-9787-8. Epub 2016 Jun 24. Forensic Sci Med Pathol. 2016. PMID: 27342771
-
The current state of forensic imaging - post mortem imaging.Int J Legal Med. 2025 May;139(3):1141-1159. doi: 10.1007/s00414-025-03461-x. Epub 2025 Mar 24. Int J Legal Med. 2025. PMID: 40126650 Free PMC article. Review.
-
Essence of postmortem computed tomography for in-hospital deaths: what clinical radiologists should know.Jpn J Radiol. 2023 Oct;41(10):1039-1050. doi: 10.1007/s11604-023-01443-w. Epub 2023 May 17. Jpn J Radiol. 2023. PMID: 37193920 Free PMC article. Review.
References
-
- Patriquin L, Kassarjian A, Barish M, Casserley L, O'Brien M, Andry C, et al. Postmortem whole-body magnetic resonance imaging as an adjunct to autopsy: preliminary clinical experience. J Magn Reson Imaging. 2001;13:277–287. - PubMed
-
- Thali MJ, Yen K, Schweitzer W, Vock P, Boesch C, Ozdoba C, et al. Virtopsy, a new imaging horizon in forensic pathology: virtual autopsy by postmortem multislice computed tomography (MSCT) and magnetic resonance imaging (MRI)--a feasibility study. J Forensic Sci. 2003;48:386–403. - PubMed
-
- Ezawa H, Yoneyama R, Kandatsu S, Yoshikawa K, Tsujii H, Harigaya K. Introduction of autopsy imaging redefines the concept of autopsy: 37 cases of clinical experience. Pathol Int. 2003;53:865–873. - PubMed
-
- Shiotani S, Kohno M, Ohashi N, Yamazaki K, Nakayama H, Watanabe K, et al. Non-traumatic postmortem computed tomographic (PMCT) findings of the lung. Forensic Sci Int. 2004;139:39–48. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
