

Imaging of Herniated Discs of the Cervical Spine: Inter-Modality Differences between 64-Slice Multidetector CT and 1.5-T MRI
- PMID: 26175589
- PMCID: PMC4499554
- DOI: 10.3348/kjr.2015.16.4.881
Imaging of Herniated Discs of the Cervical Spine: Inter-Modality Differences between 64-Slice Multidetector CT and 1.5-T MRI
Abstract
Objective: To assess inter-modality variability when evaluating cervical intervertebral disc herniation using 64-slice multidetector-row computed tomography (MDCT) and magnetic resonance imaging (MRI).
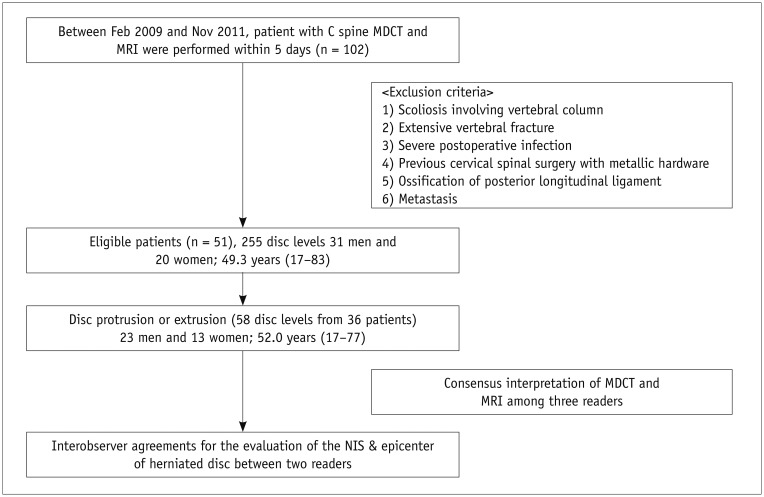
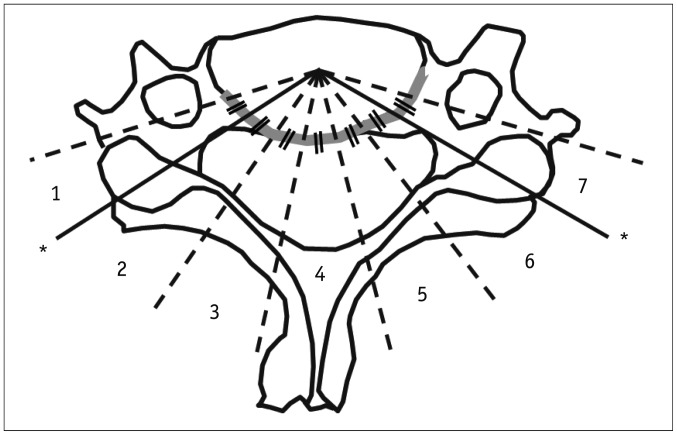
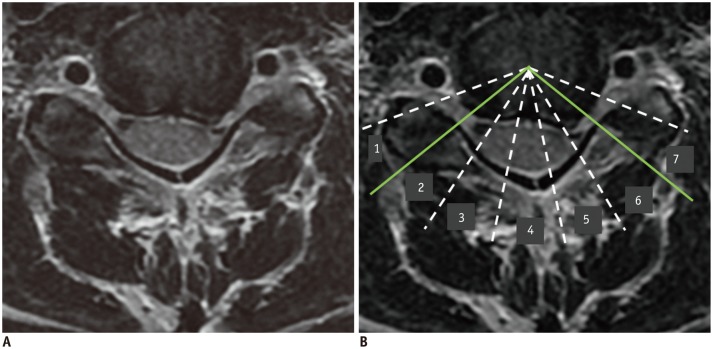
Materials and methods: Three musculoskeletal radiologists independently reviewed cervical spine 1.5-T MRI and 64-slice MDCT data on C2-3 though C6-7 of 51 patients in the context of intervertebral disc herniation. Interobserver and inter-modality agreements were expressed as unweighted kappa values. Weighted kappa statistics were used to assess the extents of agreement in terms of the number of involved segments (NIS) in disc herniation and epicenter measurements collected using MDCT and MRI.
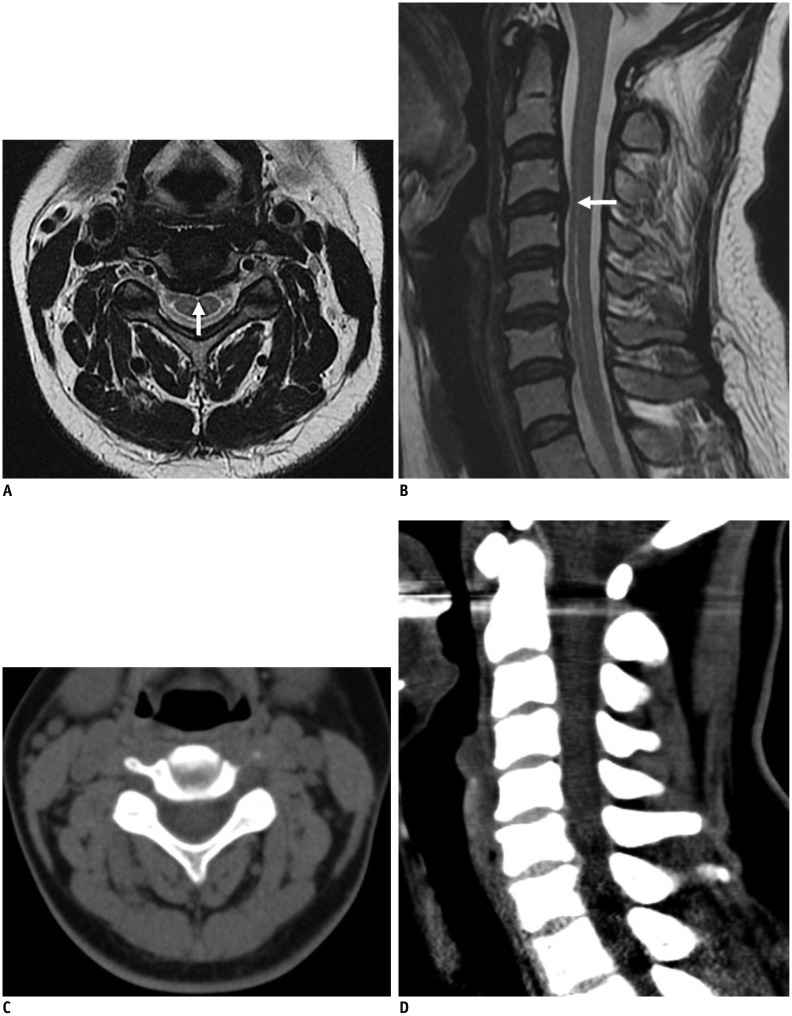
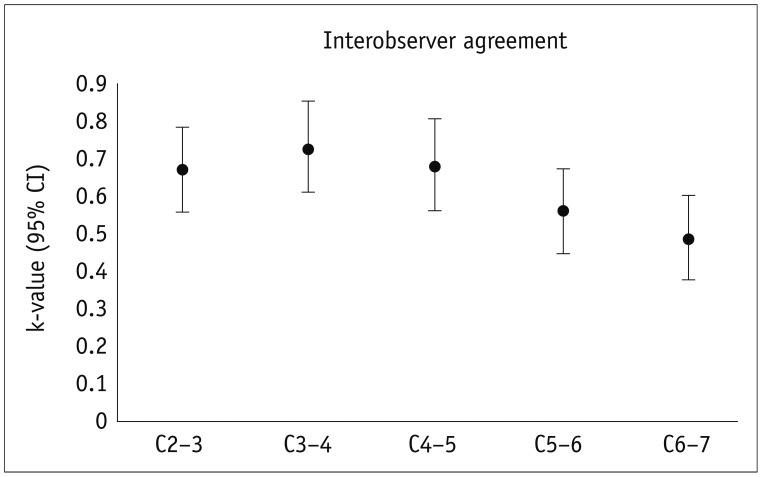
Results: The interobserver agreement rates upon evaluation of disc morphology by the three radiologists were in fair to moderate agreement (k = 0.39-0.53 for MDCT images; k = 0.45-0.56 for MRIs). When the disc morphology was categorized into two and four grades, the inter-modality agreement rates were moderate (k-value, 0.59) and substantial (k-value, 0.66), respectively. The inter-modality agreements for evaluations of the NIS (k-value, 0.78) and the epicenter (k-value, 0.79) were substantial. Also, the interobserver agreements for the NIS (CT; k-value, 0.85 and MRI; k-value, 0.88) and epicenter (CT; k-value, 0.74 and MRI; k-value, 0.70) evaluations by two readers were substantial. MDCT tended to underestimate the extent of herniated disc lesions compared with MRI.
Conclusion: Multidetector-row computed tomography and MRI showed a moderate-to-substantial degree of inter-modality agreement for the assessment of herniated cervical discs. MDCT images have a tendency to underestimate the anterior/posterior extent of the herniated disc compared with MRI.
Keywords: Cervical spine; Disc herniation; MDCT; MRI.
Figures
References
-
- Lunsford LD, Bissonette DJ, Jannetta PJ, Sheptak PE, Zorub DS. Anterior surgery for cervical disc disease. Part 1: Treatment of lateral cervical disc herniation in 253 cases. J Neurosurg. 1980;53:1–11. - PubMed
-
- Radhakrishnan K, Litchy WJ, O'Fallon WM, Kurland LT. Epidemiology of cervical radiculopathy. A population-based study from Rochester, Minnesota, 1976 through 1990. Brain. 1994;117(Pt 2):325–335. - PubMed
-
- Daniels DL, Grogan JP, Johansen JG, Meyer GA, Williams AL, Haughton VM. Cervical radiculopathy: computed tomography and myelography compared. Radiology. 1984;151:109–113. - PubMed
-
- Miyazaki M, Hong SW, Yoon SH, Morishita Y, Wang JC. Reliability of a magnetic resonance imaging-based grading system for cervical intervertebral disc degeneration. J Spinal Disord Tech. 2008;21:288–292. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
