

Quantity and Quality of Inhaled Dose Predicts Immunopathology in Tuberculosis
- PMID: 26175730
- PMCID: PMC4484340
- DOI: 10.3389/fimmu.2015.00313
Quantity and Quality of Inhaled Dose Predicts Immunopathology in Tuberculosis
Erratum in
-
Corrigendum: Quantity and Quality of Inhaled Dose Predicts Immunopathology in Tuberculosis.Front Immunol. 2015 Oct 1;6:511. doi: 10.3389/fimmu.2015.00511. eCollection 2015. Front Immunol. 2015. PMID: 26483797 Free PMC article.
Abstract
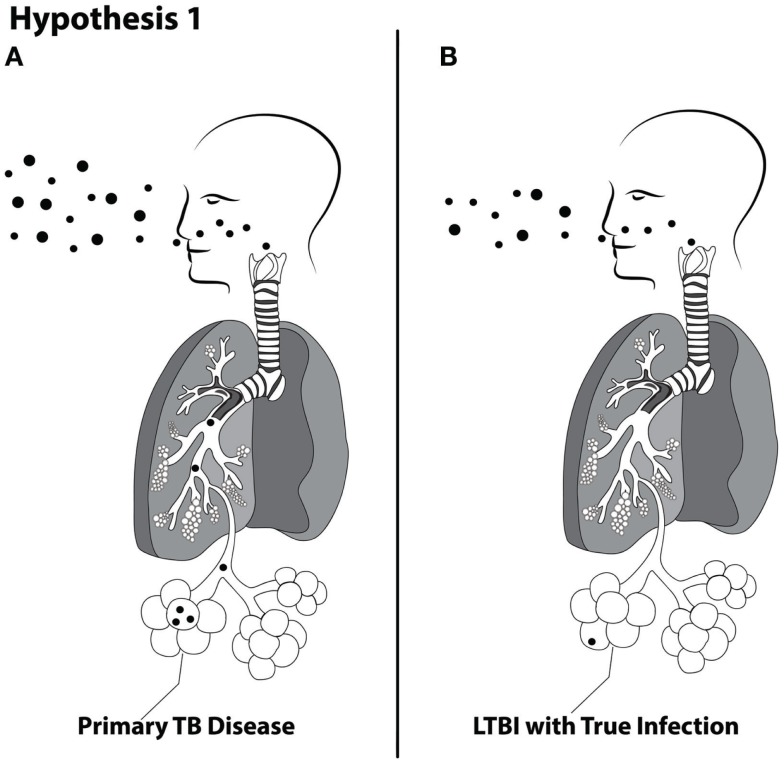
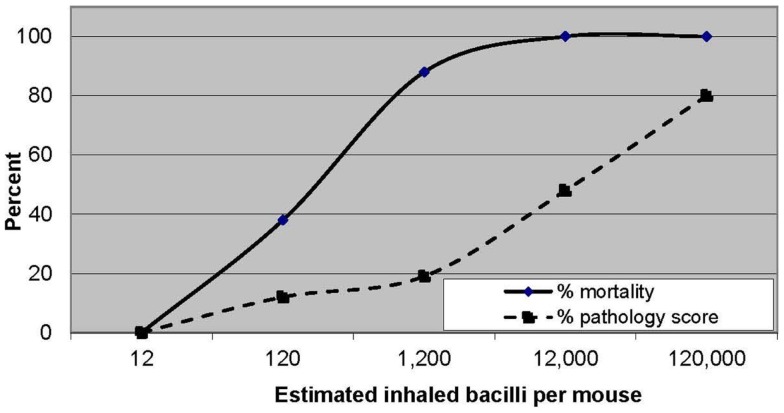
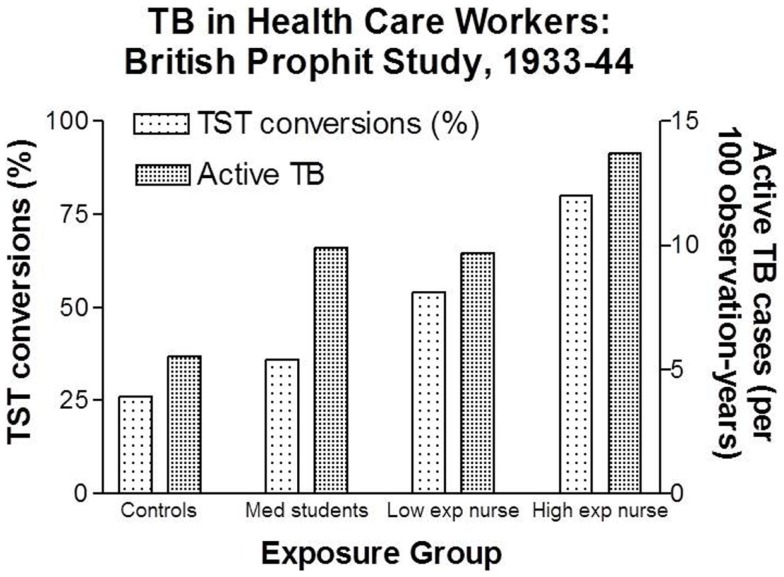
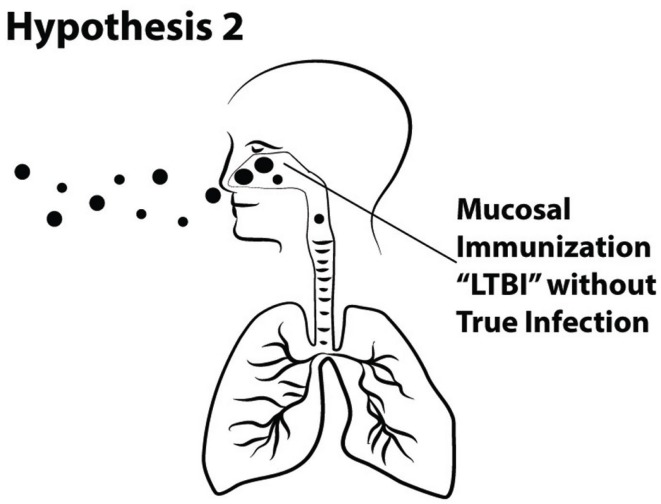
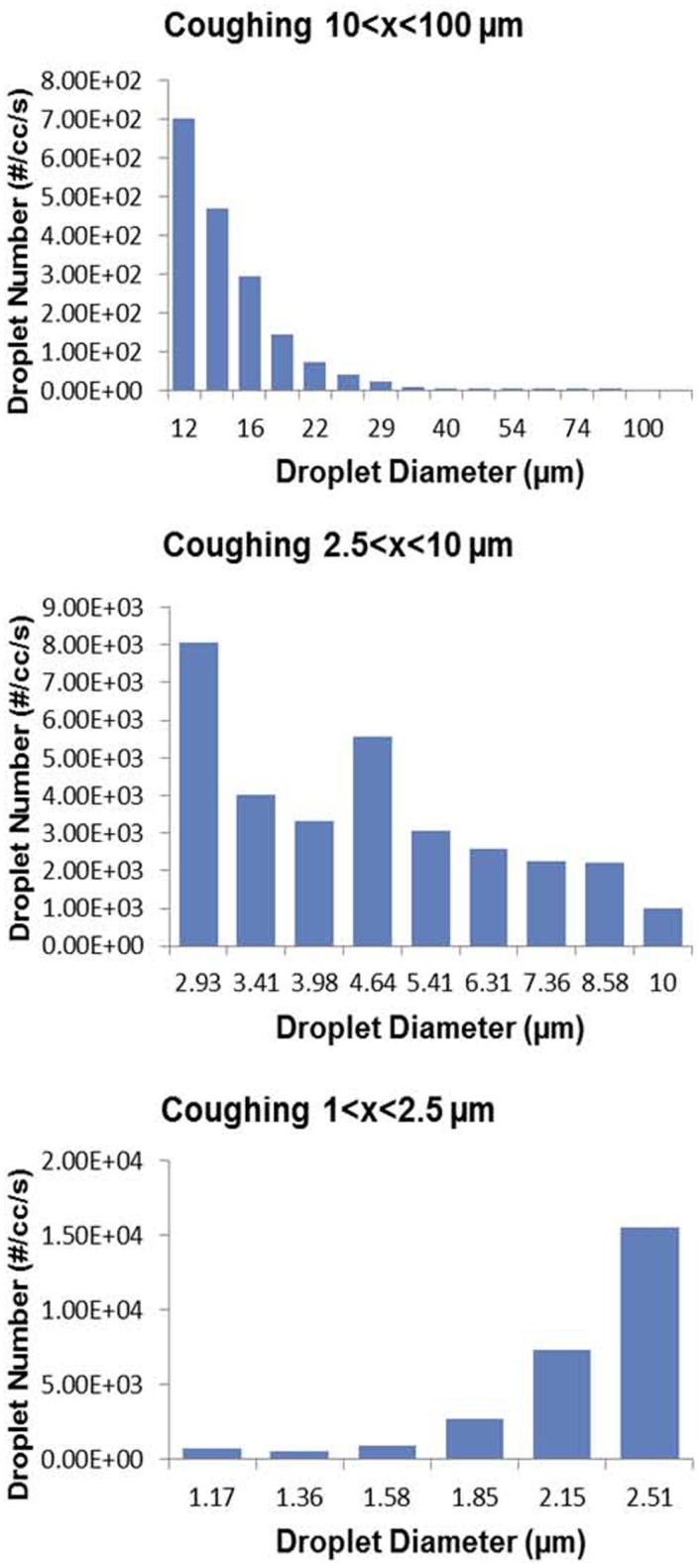
Experimental animal models of tuberculosis (TB) have convincingly demonstrated that inhaled dose predicts immunopathology and survival. In contrast, the importance of inhaled dose has generally not been appreciated in TB epidemiology, clinical science, or the practice of TB control. Infectiousness of TB patients has traditionally been assessed using microscopy for acid-fast bacilli in the sputum, which should be considered only a risk factor. We have recently demonstrated that cough aerosol cultures from index cases with pulmonary TB are the best predictors of new infection among household contacts. We suggest that cough aerosols of M. tuberculosis are the best surrogates of inhaled dose, and we hypothesize that the quantity of cough aerosols is associated with TB infection versus disease. Although several factors affect the quality of infectious aerosols, we propose that the particle size distribution of cough aerosols is an important predictor of primary upper airway disease and cervical lymphadenitis and of immune responses in exposed hosts. We hypothesize that large droplet aerosols (>5 μ) containing M. tuberculosis deposit in the upper airway and can induce immune responses without establishing infection. We suggest that this may partially explain the large proportion of humans who never develop TB disease in spite of having immunological evidence of M. tuberculosis infection (e.g., positive tuberculin skin test or interferon gamma release assay). If these hypotheses are proven true, they would alter the current paradigm of latent TB infection and reactivation, further demonstrating the need for better biomarkers or methods of assessing TB infection and the risk of developing disease.
Keywords: TB transmission; cough aerosol; immunology; inhaled dose; latent infection; tuberculosis.
Figures
Similar articles
-
What is in a cough?Int J Mycobacteriol. 2016 Dec;5 Suppl 1:S51. doi: 10.1016/j.ijmyco.2016.10.037. Epub 2016 Nov 25. Int J Mycobacteriol. 2016. PMID: 28043607
-
Cough aerosols of Mycobacterium tuberculosis predict new infection: a household contact study.Am J Respir Crit Care Med. 2013 May 1;187(9):1007-15. doi: 10.1164/rccm.201208-1422OC. Am J Respir Crit Care Med. 2013. PMID: 23306539 Free PMC article.
-
Cough-aerosol cultures of Mycobacterium tuberculosis in the prediction of outcomes after exposure. A household contact study in Brazil.PLoS One. 2018 Oct 29;13(10):e0206384. doi: 10.1371/journal.pone.0206384. eCollection 2018. PLoS One. 2018. PMID: 30372480 Free PMC article.
-
[Evolution of IGRA researches].Kekkaku. 2008 Sep;83(9):641-52. Kekkaku. 2008. PMID: 18979999 Review. Japanese.
-
[Characteristics of a diagnostic method for tuberculosis infection based on whole blood interferon-gamma assay].Kekkaku. 2006 Nov;81(11):681-6. Kekkaku. 2006. PMID: 17154047 Review. Japanese.
Cited by
-
RISK FACTORS OF LATENT TUBERCULOSIS INFECTION IN HEALTHCARE WORKERS AT HOSPITALS IN JEMBER CITY INDONESIA.Afr J Infect Dis. 2020 Dec 14;15(1):34-40. doi: 10.21010/ajid.v15i1.4. eCollection 2021. Afr J Infect Dis. 2020. PMID: 33884356 Free PMC article.
-
Whole-genome sequencing identifies nosocomial transmission of extra-pulmonary Mycobacterium tuberculosis.QJM. 2017 Sep 1;110(9):611-612. doi: 10.1093/qjmed/hcx115. QJM. 2017. PMID: 28633485 Free PMC article. No abstract available.
-
Cough Aerosols of Mycobacterium tuberculosis in the Prediction of Incident Tuberculosis Disease in Household Contacts.Clin Infect Dis. 2016 Jul 1;63(1):10-20. doi: 10.1093/cid/ciw199. Epub 2016 Mar 29. Clin Infect Dis. 2016. PMID: 27025837 Free PMC article.
-
Research Roadmap for Tuberculosis Transmission Science: Where Do We Go From Here and How Will We Know When We're There?J Infect Dis. 2017 Nov 3;216(suppl_6):S662-S668. doi: 10.1093/infdis/jix353. J Infect Dis. 2017. PMID: 29112744 Free PMC article. Review.
-
The tryptophan biosynthetic pathway is essential for Mycobacterium tuberculosis to cause disease.Biochem Soc Trans. 2020 Oct 30;48(5):2029-2037. doi: 10.1042/BST20200194. Biochem Soc Trans. 2020. PMID: 32915193 Free PMC article. Review.
References
-
- Osterholm MT, Hedberg CW. Epidemiologic principles. In: Mandell GL, Bennet JE, Dolin R, editors. Mandell, Douglas, and Bennett’s Principles and Practice of Infectious Diseases. Philadelphia, PA: Churchill Livingstone; (2009). p. 179–93.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials