

Intravenous Autologous Bone Marrow Mononuclear Cell Transplantation for Stroke: Phase1/2a Clinical Trial in a Homogeneous Group of Stroke Patients
- PMID: 26176265
- PMCID: PMC4582686
- DOI: 10.1089/scd.2015.0160
Intravenous Autologous Bone Marrow Mononuclear Cell Transplantation for Stroke: Phase1/2a Clinical Trial in a Homogeneous Group of Stroke Patients
Abstract
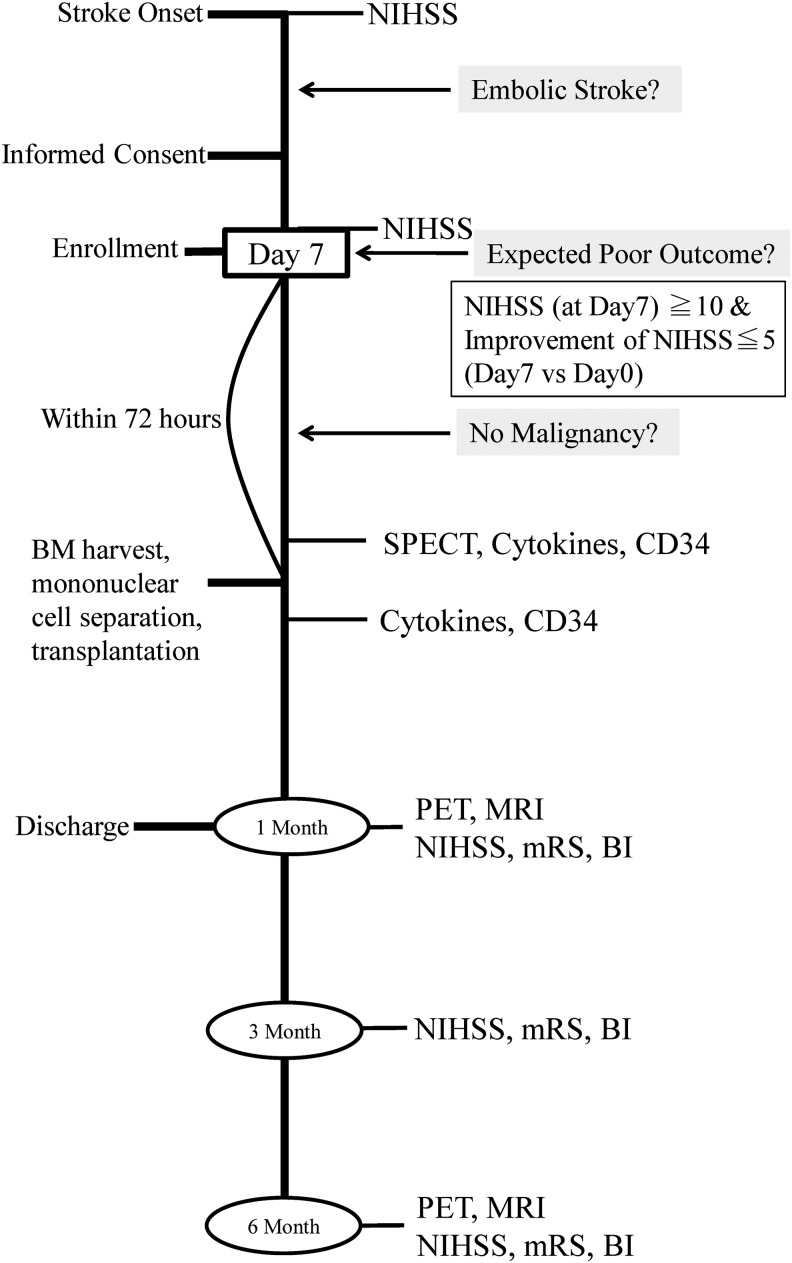
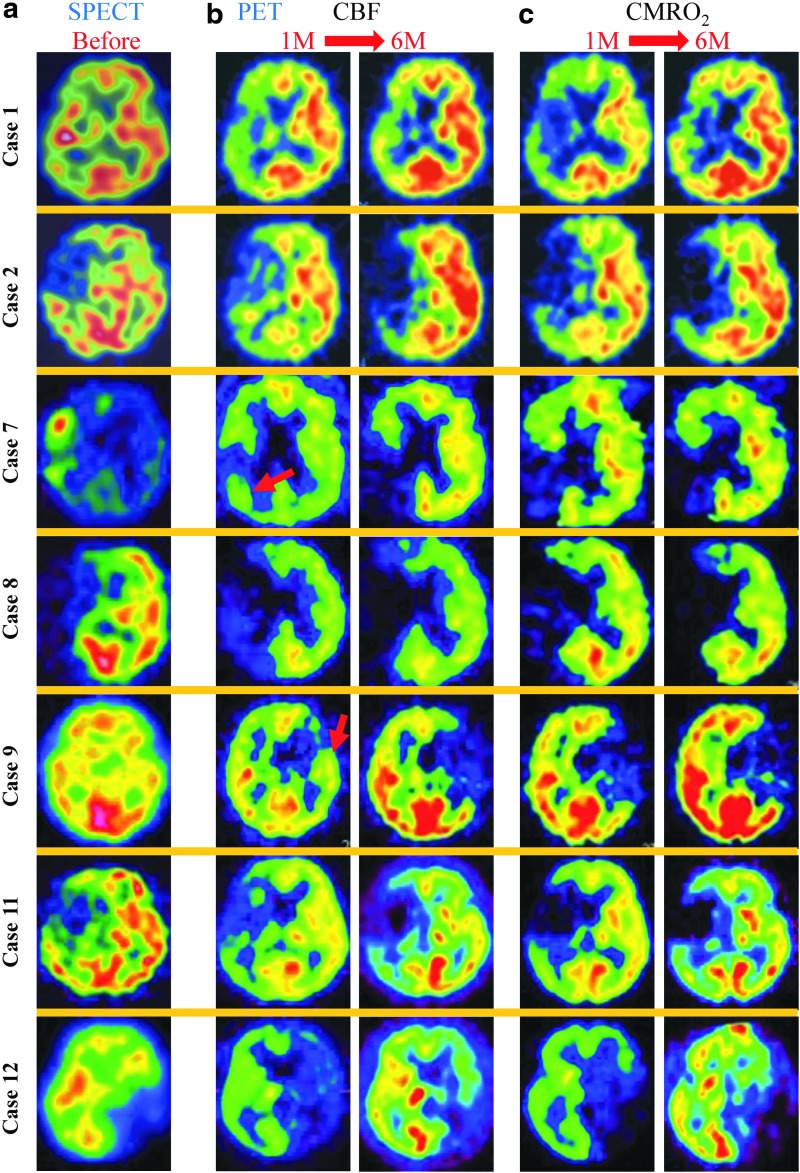
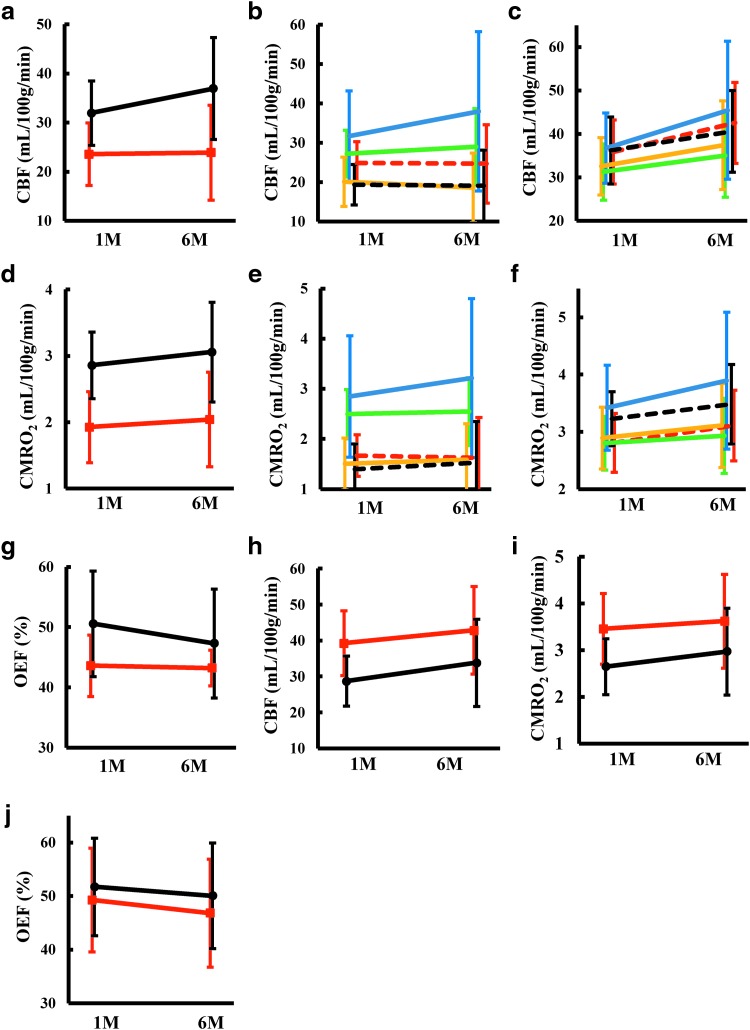
The goal of this clinical trial was to assess the feasibility and safety of transplanting autologous bone marrow mononuclear cells into patients suffering severe embolic stroke. Major inclusion criteria included patients with cerebral embolism, age 20-75 years, National Institute of Health Stroke Scale (NIHSS) score displaying improvement of ≤ 5 points during the first 7 days after stroke, and NIHSS score of ≥ 10 on day 7 after stroke. Bone marrow aspiration (25 or 50 mL; N = 6 patients in each case) was performed 7-10 days poststroke, and bone marrow mononuclear cells were administrated intravenously. Mean total transplanted cell numbers were 2.5 × 10(8) and 3.4 × 10(8) cells in the lower and higher dose groups, respectively. No apparent adverse effects of administering bone marrow cells were observed. Compared with the lower dose, patients receiving the higher dose of bone marrow cells displayed a trend toward improved neurologic outcomes. Compared with 1 month after treatment, patients receiving cell therapy displayed a trend toward improved cerebral blood flow and metabolic rate of oxygen consumption 6 months after treatment. In comparison with historical controls, patients receiving cell therapy had significantly better neurologic outcomes. Our results indicated that intravenous transplantation of autologous bone marrow mononuclear cells is safe and feasible. Positive results and trends favoring neurologic recovery and improvement in cerebral blood flow and metabolism by cell therapy underscore the relevance of larger scale randomized controlled trials using this approach.
Figures



References
-
- Pearson TA. (1999). Cardiovascular disease in developing countries: myths, realities, and opportunities. Cardiovasc Drugs Ther 13:95–104 - PubMed
-
- Goyal M, Demchuk AM, Menon BK, Eesa M, Rempel JL, Thornton J, Roy D, Jovin TG, Willinsky RA, et al. (2015). Randomized assessment of rapid endovascular treatment of ischemic stroke. N Engl J Med 372:1019–1030 - PubMed
-
- Taguchi A, Matsuyama T, Moriwaki H, Hayashi T, Hayashida K, Nagatsuka K, Todo K, Mori K, Stern DM, Soma T. and Naritomi H. (2004). Circulating CD34-positive cells provide an index of cerebrovascular function. Circulation 109:2972–2975 - PubMed
-
- Yoshihara T, Taguchi A, Matsuyama T, Shimizu Y, Kikuchi-Taura A, Soma T, Stern DM, Yoshikawa H, Kasahara Y, et al. (2008). Increase in circulating CD34-positive cells in patients with angiographic evidence of moyamoya-like vessels. J Cereb Blood Flow Metab 28:1086–1089 - PubMed
-
- Taguchi A, Matsuyama T, Nakagomi T, Shimizu Y, Fukunaga R, Tatsumi Y, Yoshikawa H, Kikuchi-Taura A, Soma T, et al. (2008). Circulating CD34-positive cells provide a marker of vascular risk associated with cognitive impairment. J Cereb Blood Flow Metab 28:445–449 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical