

Comparison of maternal and fetal outcomes among patients undergoing cesarean section under general and spinal anesthesia: a randomized clinical trial
- PMID: 26176927
- PMCID: PMC10876380
- DOI: 10.1590/1516-3180.2014.8901012
Comparison of maternal and fetal outcomes among patients undergoing cesarean section under general and spinal anesthesia: a randomized clinical trial
Abstract
Context and objective: As the rates of cesarean births have increased, the type of cesarean anesthesia has gained importance. Here, we aimed to compare the effects of general and spinal anesthesia on maternal and fetal outcomes in term singleton cases undergoing elective cesarean section.
Design and setting: Prospective randomized controlled clinical trial in a tertiary-level public hospital.
Methods: Our study was conducted on 100 patients who underwent cesarean section due to elective indications. The patients were randomly divided into general anesthesia (n = 50) and spinal anesthesia (n = 50) groups. The maternal pre and postoperative hematological results, intra and postoperative hemodynamic parameters and perinatal results were compared between the groups.
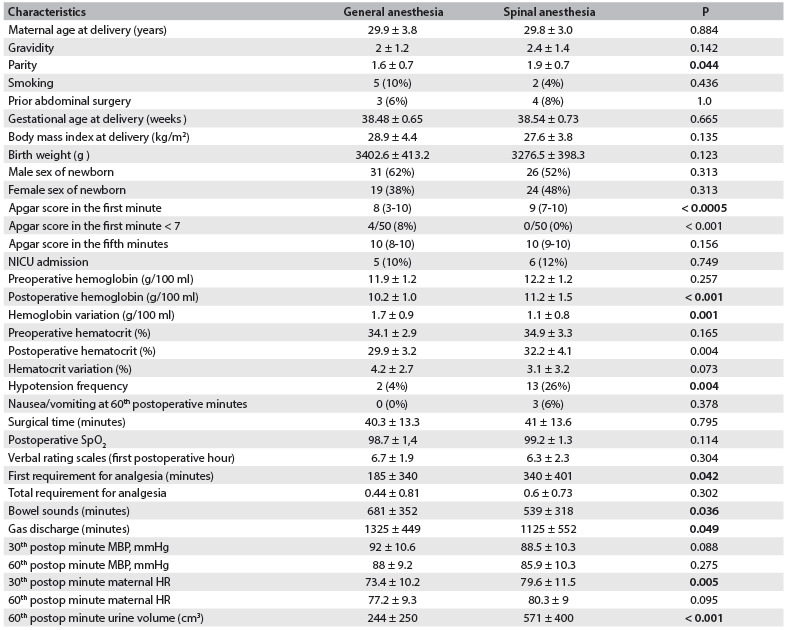
Results: Mean bowel sounds (P = 0.036) and gas discharge time (P = 0.049) were significantly greater and 24th hour hemoglobin difference values (P = 0.001) were higher in the general anesthesia group. The mean hematocrit and hemoglobin values at the 24th hour (P = 0.004 and P < 0.001, respectively), urine volume at the first postoperative hour (P < 0.001) and median Apgar score at the first minute (P < 0.0005) were significantly higher, and the time that elapsed until the first requirement for analgesia was significantly longer (P = 0.042), in the spinal anesthesia group.
Conclusion: In elective cases, spinal anesthesia is superior to general anesthesia in terms of postoperative comfort. In pregnancies with a risk of fetal distress, it would be appropriate to prefer spinal anesthesia by taking the first minute Apgar score into account.
CONTEXTO E OBJETIVO:: Como as taxas de partos cesáreos aumentaram, o tipo de anestesia na cesariana ganhou importância. Comparamos os efeitos da anestesia geral e da raquianestesia sobre os resultados maternos e fetais em casos de gestação única e no termo, com cesariana eletiva.
TIPO DE ESTUDO E LOCAL:: Ensaio clínico prospectivo, randomizado e controlado, em hospital público terciário.
MÉTODOS:: Estudo realizado com 100 pacientes que se submeteram a cesariana por indicação eletiva. As pacientes foram divididos aleatoriamente em grupos recebendo anestesia geral (n = 50) e raquianestesia (n = 50). Resultados maternos hematológicos pré e pós-operatórios, variáveis hemodinâmicas intra e pós-operatórias e resultados perinatais foram comparados entre os grupos.
RESULTADOS:: As médias de ruídos intestinais (P = 0,036) e tempo de descarga de gás (P = 0,049) foram significativamente mais elevadas e os valores de diferença de hemoglobina na 24a hora (P = 0,001) foram maiores no grupo anestesia geral. Os valores médios de hematócrito e hemoglobina na 24a hora (P = 0,004 e P < 0,001, respectivamente), o volume de urina na primeira hora de pós-operatório (P < 0,001) e a pontuação mediana de Apgar no primeiro minuto (P < 0,0005) foram significativamente maiores, e o tempo até o primeiro requerimento de analgésicos também foi significativamente maior (P = 0,042) no grupo raquianestesia.
CONCLUSÃO:: Nos casos eletivos, raquianestesia é superior à anestesia geral em termos de conforto pós-operatório. Em gestações com risco de sofrimento fetal, seria adequado preferir raquianestesia, levando em conta o Apgar no primeiro minuto.
REGISTRO DE ENSAIO CLÍNICO:: NTR17990
Conflict of interest statement
Figures
References
-
- Gori F, Pasqualucci A, Corradetti F, Milli M, Peduto VA. Maternal and neonatal outcome after cesarean section: the impact of anesthesia. J Matern Fetal Neonatal Med. 2007;20(1):53–57. - PubMed
-
- Ronsmans C, Graham WJ, Lancet Maternal Survival Series steering group Maternal mortality: who, when, where, and why. Lancet. 2006;368(9542):1189–1200. - PubMed
-
- Tsen LC. Anesthesia for cesarean section. In: Chestnut DH, Polley LS, Wong CA, Tsen LC, editors. Chestnut’s obstetric anesthesia: principles and practice. 4. Philadelphia: Elsevier Mosby; 2009. pp. 521–551.
-
- Cooper MG, McClure JH. Lewis G, Drife J. Why mothers die 2000-2002. Confidential enquiries into maternal and child health. Improving care for mothers, babies and children. London: RCOG Press; 2004. Anaesthesia; pp. 122–133.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
