

Visualizing Risk Prediction Models
- PMID: 26176945
- PMCID: PMC4503430
- DOI: 10.1371/journal.pone.0132614
Visualizing Risk Prediction Models
Abstract
Objective: Risk prediction models can assist clinicians in making decisions. To boost the uptake of these models in clinical practice, it is important that end-users understand how the model works and can efficiently communicate its results. We introduce novel methods for interpretable model visualization.
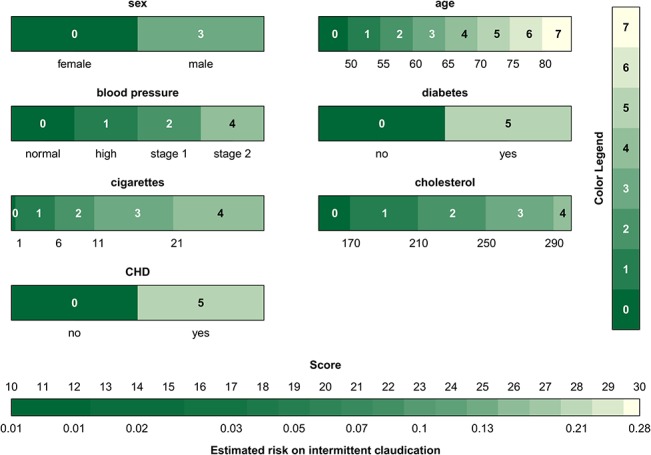
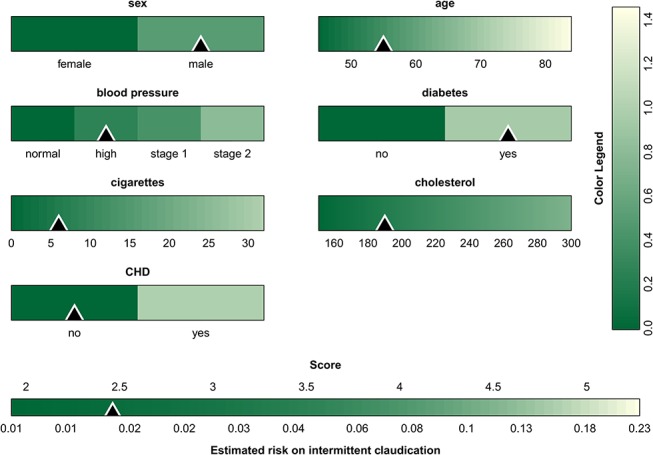
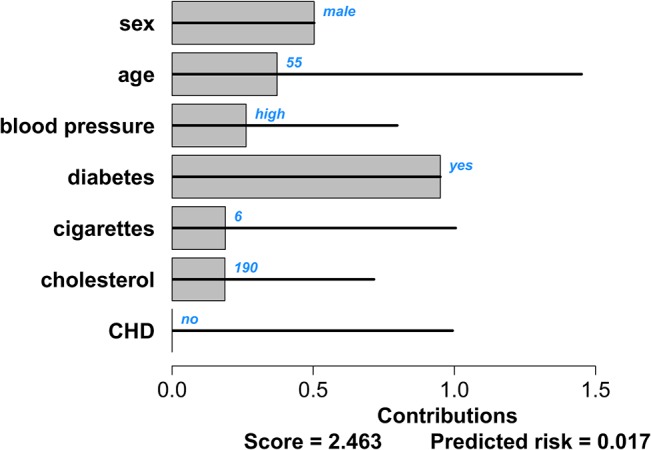
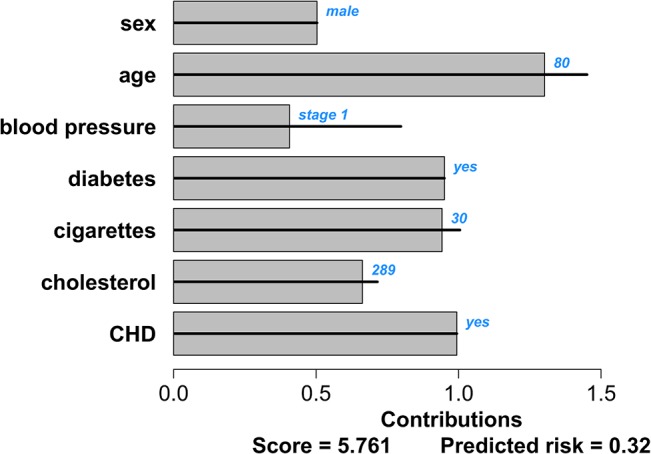
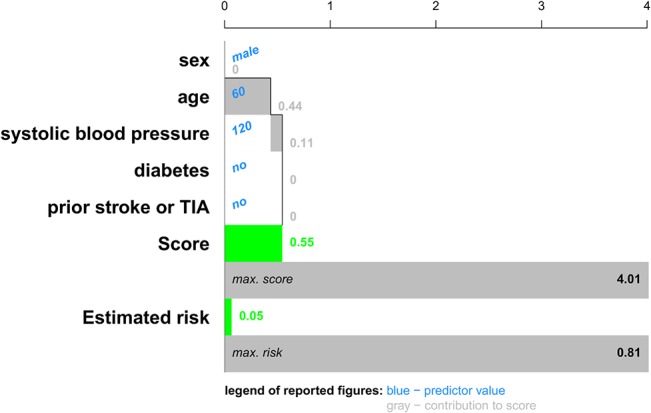
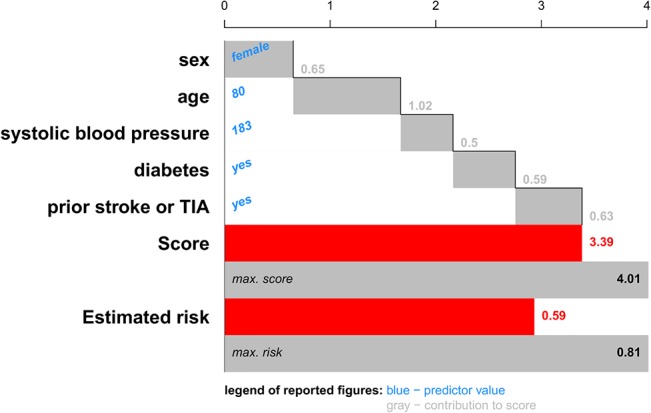
Methods: The proposed visualization techniques are applied to two prediction models from the Framingham Heart Study for the prediction of intermittent claudication and stroke after atrial fibrillation. We represent models using color bars, and visualize the risk estimation process for a specific patient using patient-specific contribution charts.
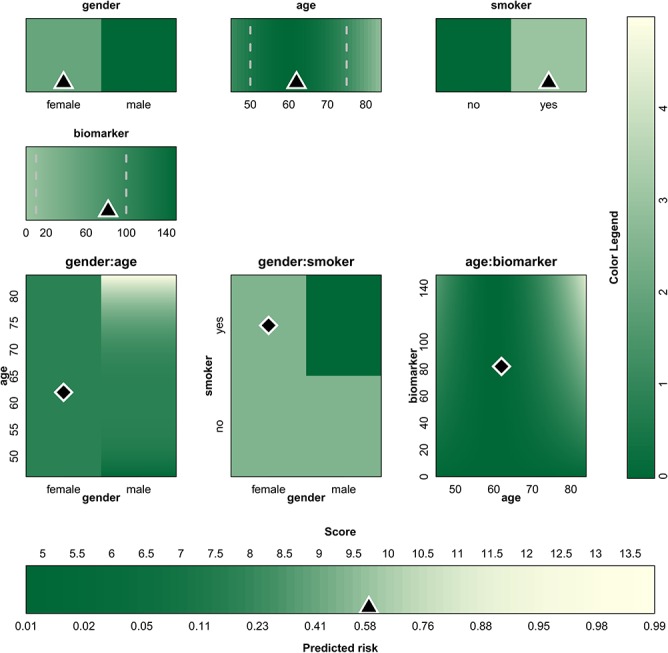
Results: The color-based model representations provide users with an attractive tool to instantly gauge the relative importance of the predictors. The patient-specific representations allow users to understand the relative contribution of each predictor to the patient's estimated risk, potentially providing insightful information on which to base further patient management. Extensions towards non-linear models and interactions are illustrated on an artificial dataset.
Conclusion: The proposed methods summarize risk prediction models and risk predictions for specific patients in an alternative way. These representations may facilitate communication between clinicians and patients.
Conflict of interest statement
Figures

References
-
- Galea M, Blamey R, Elston C, Ellis I. The Nottingham Prognostic Index in primary breast cancer. Breast Cancer Res Treat. 1992; 22(3):207–219. - PubMed
-
- Knaus WA, Wagner DP, Draper EA, Zimmerman JE, Bergner M, Bastos PG, et al. The APACHE III prognostic system. Risk prediction of hospital mortality for critically ill hospitalized adults. Chest. 1991; 100(6):1619–1636. - PubMed
-
- Timmerman D, Testa AC, Bourne T, Ferrazzi E, Ameye L, Konstantinovic ML, et al. Logistic regression model to distinguish between the benign and malignant adnexal mass before surgery: a multicenter study by the International Ovarian tumor Analysis Group. J Clin Oncol. 2005; 23(34):8794–8801. - PubMed
-
- Nashef S A, Roques F, Michel P, Gauducheau E, Lemeshow S, Salamon R. European system for cardiac operative risk evaluation (EuroSCORE). Eur J Cardiothorac Surg. 1999; 16(1):9–13. - PubMed
-
- Chalmers J, Pullan M, Fabri BM, McShane J, Shaw M, Mediratta N, et al. Validation of EuroSCORE II in a modern cohort of patients undergoing cardiac surgery. Eur J CardioThorac Surg. 2013; 43(4):688–694. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
