

Long-term Outcomes After Liver Transplantation Among Human Immunodeficiency Virus-Infected Recipients
- PMID: 26177090
- PMCID: PMC4684452
- DOI: 10.1097/TP.0000000000000829
Long-term Outcomes After Liver Transplantation Among Human Immunodeficiency Virus-Infected Recipients
Abstract
Background: Early outcomes after human immunodeficiency virus (HIV) + liver transplantation (LT) are encouraging, but data are lacking regarding long-term outcomes and comparisons with matched HIV- patients.
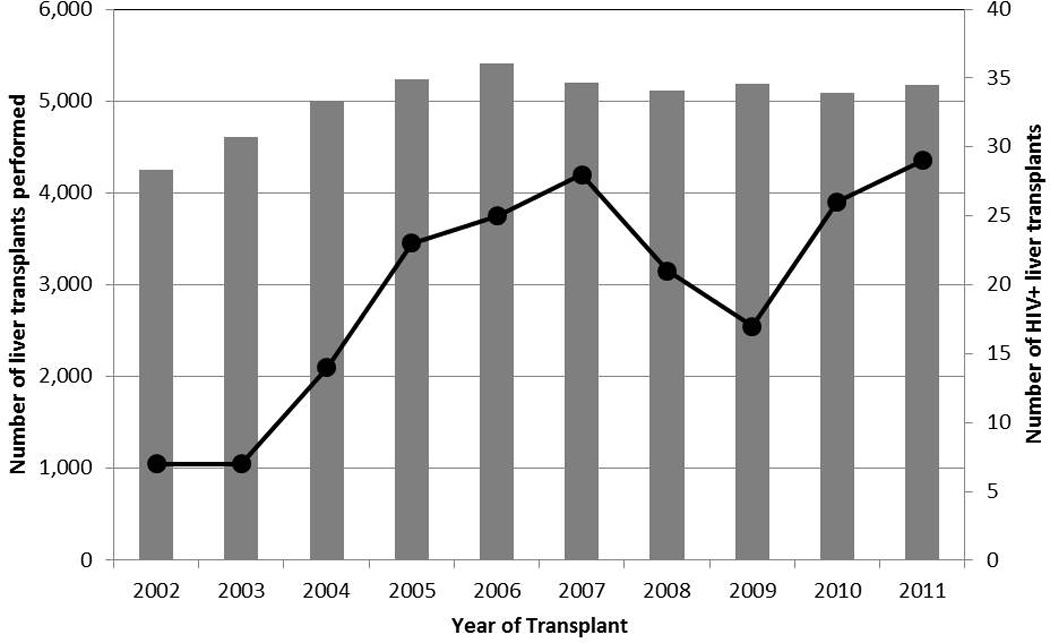
Methods: We examined outcomes among 180 HIV+ LT, and compared outcomes to matched HIV- counterfactuals (Scientific Registry of Transplant Recipients 2002-2011). Iterative expanding radius matching (1:10) on recipient age, race, body mass index, hepatitis C virus (HCV), model for end-stage liver disease score, and acute rejection; and donor age and race, cold ischemia time, and year of transplant. Patient survival and graft survival were estimated using Kaplan-Meier methodology and compared using log-rank and Cox proportional hazards. Subgroup analyses were performed by transplant era (early: 2002-2007 vs. modern: 2008-2011) and HCV infection status.
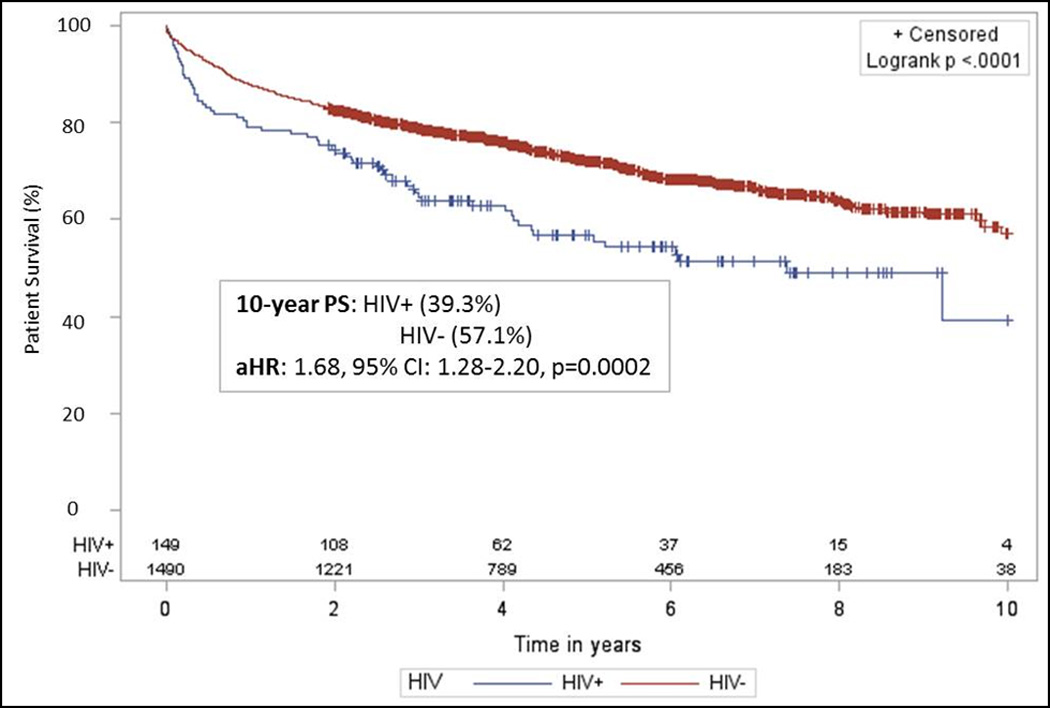
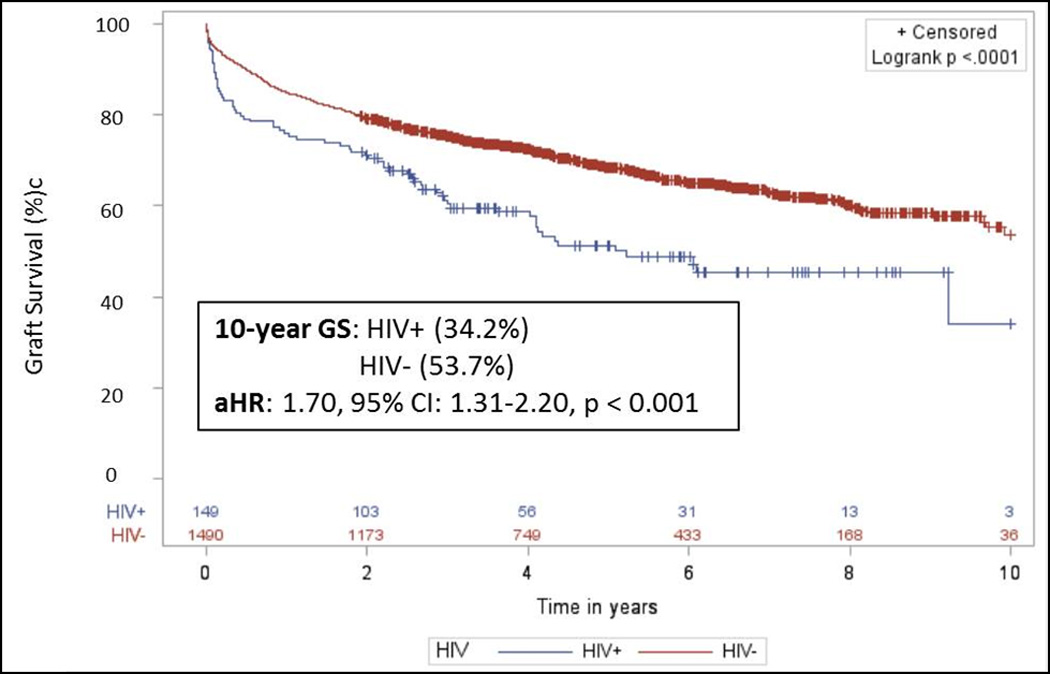
Results: Compared to matched HIV- controls, HIV+ LT recipients had a 1.68-fold increased risk for death (adjusted hazard ratio [aHR], 1.68, 95% confidence interval [95% CI], 1.28-2.20; P < 0.001), and a 1.70-fold increased risk for graft loss (aHR, 1.70; 95% CI, 1.31-2.20; P < 0.001). These differences persisted independent of HCV infection status. However, in the modern transplant era risk for death (aHR, 1.11; 95% CI, 0.52-2.35; P = 0.79) and graft loss (aHR, 0.89; 95% CI, 0.42-1.88; P = 0.77) were similar between monoinfected and uninfected LT recipients. In contrast, independent of transplant era, coinfected LT recipients had increased risk for death (aHR, 2.24; 95% CI, 1.43-3.53; P < 0.001) and graft loss (aHR, 2.07; 95% CI, 1.33-3.22; P = 0.001) compared to HCV+ alone LT recipients.
Conclusions: These results suggest that outcomes among monoinfected HIV+ LT recipients have improved over time. However, outcomes among HIV+ LT recipients coinfected with HCV remain concerning and motivate future survival benefit studies.
Conflict of interest statement
Figures
References
-
- [June 9, 2014];HIV in the United States: A Glance. 2013 Available from: http://www.cdc.gov/hiv/statistics/basics/ataglance.html.
-
- Palella FJ, Jr, Delaney KM, Moorman AC, et al. Declining morbidity and mortality among patients with advanced human immunodeficiency virus infection. HIV Outpatient Study Investigators. N Engl J Med. 1998;338(13):853–860. - PubMed
-
- Rao TK. Human immunodeficiency virus infection in end-stage renal disease patients. Semin Dial. 2003;16(3):233–244. - PubMed
-
- Blumberg EA, Stock P Practice ASTIDCo. Solid organ transplantation in the HIV-infected patient. American journal of transplantation : official journal of the American Society of Transplantation and the American Society of Transplant Surgeons. 2009;9(Suppl 4):S131–S135. - PubMed
-
- Stock PG, Roland ME. Evolving clinical strategies for transplantation in the HIV-positive recipient. Transplantation. 2007;84(5):563–571. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
