

Sleep Disorders in Parkinsonian and Nonparkinsonian LRRK2 Mutation Carriers
- PMID: 26177462
- PMCID: PMC4503402
- DOI: 10.1371/journal.pone.0132368
Sleep Disorders in Parkinsonian and Nonparkinsonian LRRK2 Mutation Carriers
Abstract
Objective: In idiopathic Parkinson disease (IPD) sleep disorders are common and may antedate the onset of parkinsonism. Based on the clinical similarities between IPD and Parkinson disease associated with LRRK2 gene mutations (LRRK2-PD), we aimed to characterize sleep in parkinsonian and nonmanifesting LRRK2 mutation carriers (NMC).
Methods: A comprehensive interview conducted by sleep specialists, validated sleep scales and questionnaires, and video-polysomnography followed by multiple sleep latency test (MSLT) assessed sleep in 18 LRRK2-PD (17 carrying G2019S and one R1441G mutations), 17 NMC (11 G2019S, three R1441G, three R1441C), 14 non-manifesting non-carriers (NMNC) and 19 unrelated IPD.
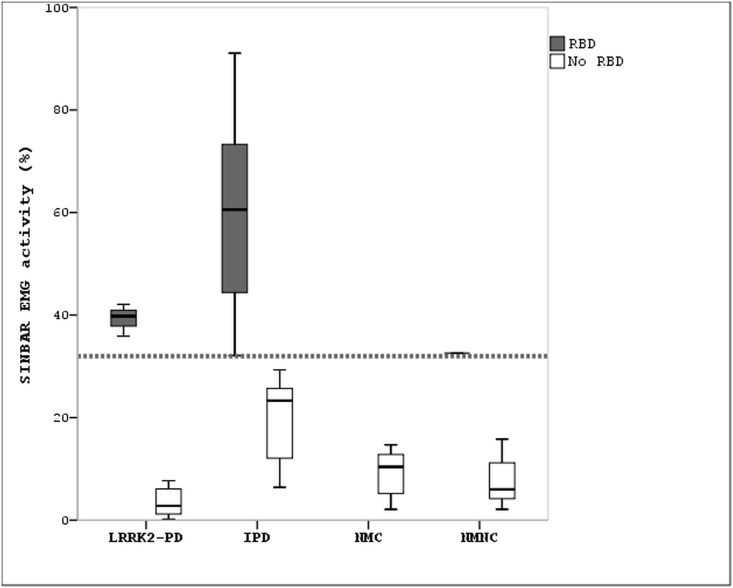
Results: Sleep complaints were frequent in LRRK2-PD patients; 78% reported poor sleep quality, 33% sleep onset insomnia, 56% sleep fragmentation and 39% early awakening. Sleep onset insomnia correlated with depressive symptoms and poor sleep quality. In LRRK2-PD, excessive daytime sleepiness (EDS) was a complaint in 33% patients and short sleep latencies on the MSLT, which are indicative of objective EDS, were found in 71%. Sleep attacks occurred in three LRRK2-PD patients and a narcoleptic phenotype was not observed. REM sleep behavior disorder (RBD) was diagnosed in three LRRK2-PD. EDS and RBD were always reported to start after the onset of parkinsonism in LRRK2-PD. In NMC, EDS was rarely reported and RBD was absent. When compared to IPD, sleep onset insomnia was more significantly frequent, EDS was similar, and RBD was less significantly frequent and less severe in LRRK2-PD. In NMC, RBD was not detected and sleep complaints were much less frequent than in LRRK2-PD. No differences were observed in sleep between NMC and NMNC.
Conclusions: Sleep complaints are frequent in LRRK2-PDand show a pattern that when compared to IPD is characterized by more frequent sleep onset insomnia, similar EDS and less prominent RBD. Unlike in IPD, RBD and EDS seem to be not markers of the prodromal stage of LRRK2-PD.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
