

Chemotherapy responsiveness in a patient with multiply relapsed ameloblastic fibro-odontosarcoma of the maxilla
- PMID: 26178860
- PMCID: PMC4737202
- DOI: 10.1002/pbc.25627
Chemotherapy responsiveness in a patient with multiply relapsed ameloblastic fibro-odontosarcoma of the maxilla
Abstract
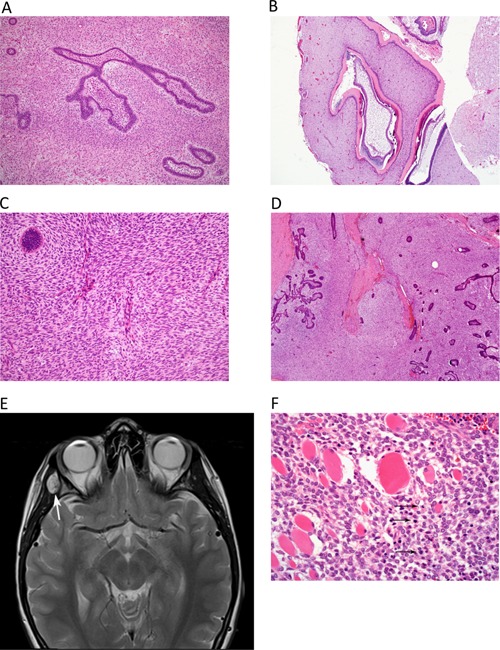
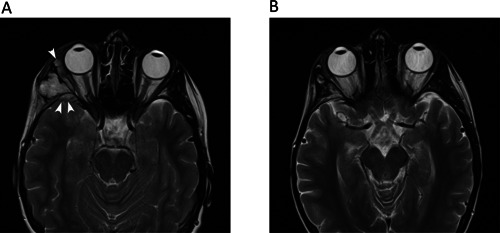
Ameloblastic fibro-odontosarcoma (AFOS) is an extremely rare malignant odontogenic tumor. Complete surgical excision is the treatment of choice. Deaths due to disease recurrence and/or progression are documented. Here, we report the case of a 15-year-old female with multiple recurrent AFOS. She responded to chemotherapy with ifosfamide and doxorubicin consolidated by stereotactic reirradiation using cyberknife and remained in complete remission 14 months from the end of reirradiation therapy. Chemotherapy with ifosfamide and doxorubicin should be considered in advanced cases of AFOS.
Keywords: ameloblastic fibro-odontoma; ameloblastic fibro-odontosarcoma; chemotherapy response; radiotherapy; relapse; transformation.
© 2015 The Authors. Pediatric Blood & Cancer Published by Wiley Periodicals, Inc.
Figures
Similar articles
-
Ameloblastic fibro-odontosarcoma of the mandible with active epithelial proliferation: A rare case report.Mol Clin Oncol. 2017 Dec;7(6):971-975. doi: 10.3892/mco.2017.1448. Epub 2017 Oct 12. Mol Clin Oncol. 2017. PMID: 29285358 Free PMC article.
-
Ameloblastic fibro-odontosarcoma: a case report.Int J Oral Maxillofac Surg. 2009 Mar;38(3):289-92. doi: 10.1016/j.ijom.2008.11.025. Epub 2009 Jan 15. Int J Oral Maxillofac Surg. 2009. PMID: 19150219
-
Ameloblastic fibro-odontosarcoma of the mandible in a pediatric patient.Eur Ann Otorhinolaryngol Head Neck Dis. 2016 Dec;133(6):419-421. doi: 10.1016/j.anorl.2015.11.010. Epub 2016 Apr 26. Eur Ann Otorhinolaryngol Head Neck Dis. 2016. PMID: 27130809
-
Ameloblastic carcinoma of the maxilla: case report and review of the literature.Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007 Dec;104(6):e17-24. doi: 10.1016/j.tripleo.2007.05.026. Epub 2007 Oct 17. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007. PMID: 17942338 Review.
-
Ameloblastic fibrodentinosarcoma and ameloblastic fibro-odontosarcoma: A systematic review.J Stomatol Oral Maxillofac Surg. 2018 Nov;119(5):401-406. doi: 10.1016/j.jormas.2018.03.007. Epub 2018 Mar 21. J Stomatol Oral Maxillofac Surg. 2018. PMID: 29574112
Cited by
-
Odontogenic Sarcomas of the Mandible.Biomedicines. 2024 Mar 8;12(3):615. doi: 10.3390/biomedicines12030615. Biomedicines. 2024. PMID: 38540228 Free PMC article.
-
Clinical management of primary odontogenic sarcoma in the mandible: a case report after WHO nomination.J Biomed Res. 2022 Jan 28;36(1):58-62. doi: 10.7555/JBR.35.20210133. J Biomed Res. 2022. PMID: 35403611 Free PMC article.
-
Ameloblastic fibrosarcoma of the maxilla arising in an old woman, a rare case report and literature review.BMC Oral Health. 2024 Jun 27;24(1):743. doi: 10.1186/s12903-024-04509-x. BMC Oral Health. 2024. PMID: 38937725 Free PMC article. Review.
-
A mixed odontogenic sarcoma: A challenging histopathologic case and brief review of the literature.J Oral Maxillofac Pathol. 2018 Jan;22(Suppl 1):S29-S34. doi: 10.4103/jomfp.JOMFP_74_17. J Oral Maxillofac Pathol. 2018. PMID: 29491601 Free PMC article.
-
Ameloblastic fibro-odontosarcoma of the mandible with active epithelial proliferation: A rare case report.Mol Clin Oncol. 2017 Dec;7(6):971-975. doi: 10.3892/mco.2017.1448. Epub 2017 Oct 12. Mol Clin Oncol. 2017. PMID: 29285358 Free PMC article.
References
-
- Carlos R, Alini M, Takeda Y. Odontogenic sarcomas In: Barnes L, Eveson J, Reichart P, Sidransky D, editors. Pathology and genetics of head and neck tumours. Lyon: IARC Press; 2005. p. 294–295.
-
- Goldstein G, Parker FP, Hugh GS. Ameloblastic sarcoma: Pathogenesis and treatment with chemotherapy. Cancer 1976; 37:1673–1678. - PubMed
-
- Minard‐Colin V, Cassagneau E, Supiot S, Oberlin O, D'hautuille C, Corradini N. Ameloblastic fibrosarcoma of the mandible: Report of 2 chemosensitive pediatric cases. J Pediatr Hematol Oncol 2012; 34:e72–e76. - PubMed
-
- Takeda Y, Kuroda M, Suzuki A. Ameloblastic odontosarcoma (ameloblastic fibro‐odontosarcoma) in the mandible. Acta Pathol Jpn 1990; 40:832–837. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
