

Histone deacetylase inhibition sensitizes osteosarcoma to heavy ion radiotherapy
- PMID: 26178881
- PMCID: PMC4504102
- DOI: 10.1186/s13014-015-0455-z
Histone deacetylase inhibition sensitizes osteosarcoma to heavy ion radiotherapy
Abstract
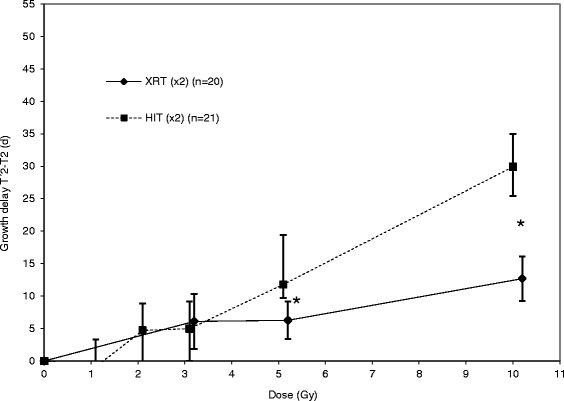
Background: Minimal improvements in treatment or survival of patients with osteosarcoma have been achieved during the last three decades. Especially in the case of incomplete tumor resection, prognosis remains poor. Heavy ion radiotherapy (HIT) and modern anticancer drugs like histone deacetylase inhibitors (HDACi) have shown promising effects in osteosarcoma in vitro. In this study, we tested the effect of HIT and the combination of HIT and the HDACi suberoylanilide hydroxamic acid (SAHA) in a xenograft mouse model.
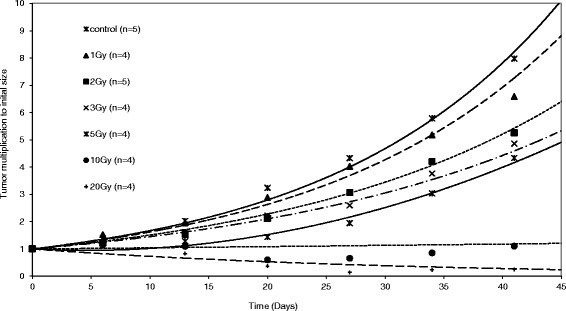
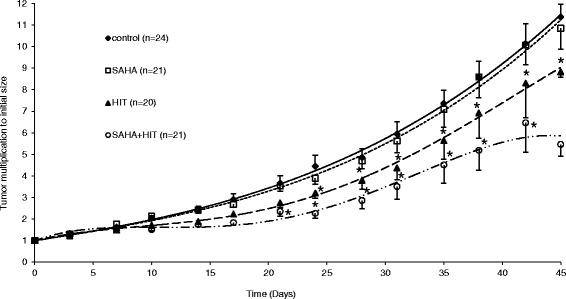
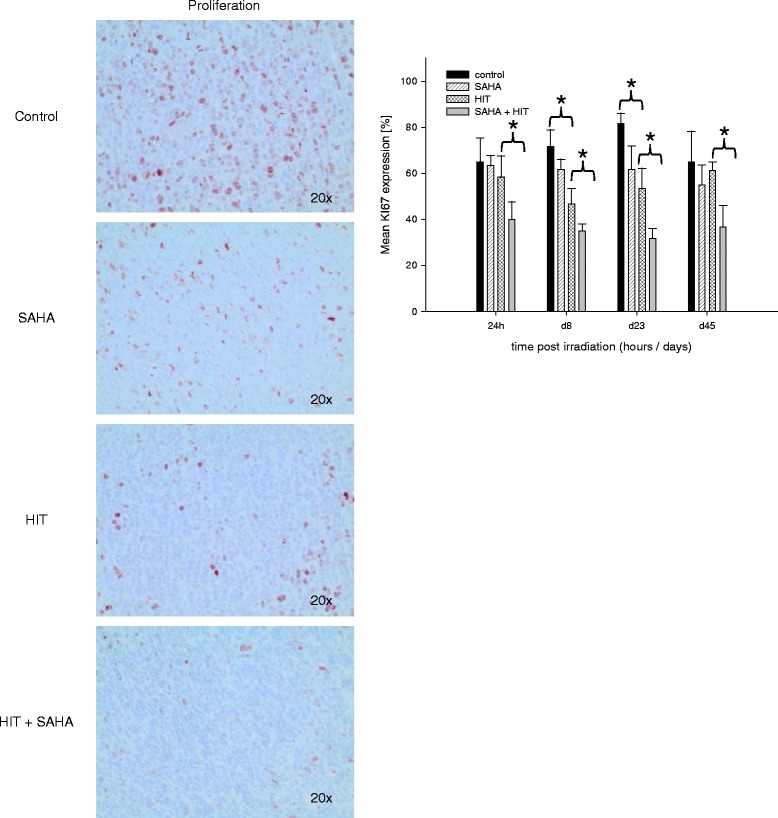
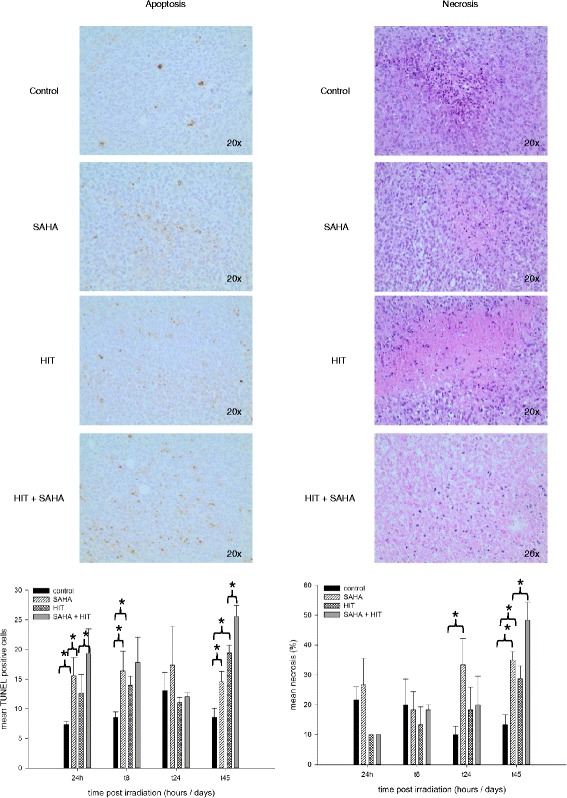
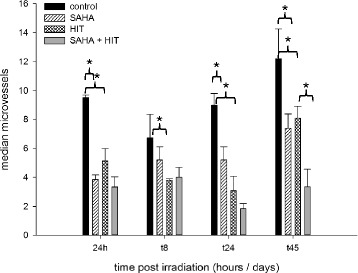
Methods: Osteosarcoma xenografts were established by subcutaneous injection of KHOS-24OS cells and treated with either vehicle (DMSO), SAHA, HIT or HIT and SAHA. Tumor growth was determined and tumor necrosis, proliferation rate, apoptotic rate as well as vessel density were evaluated.
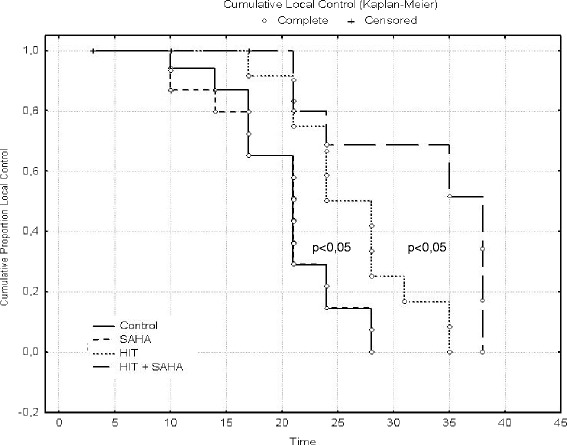
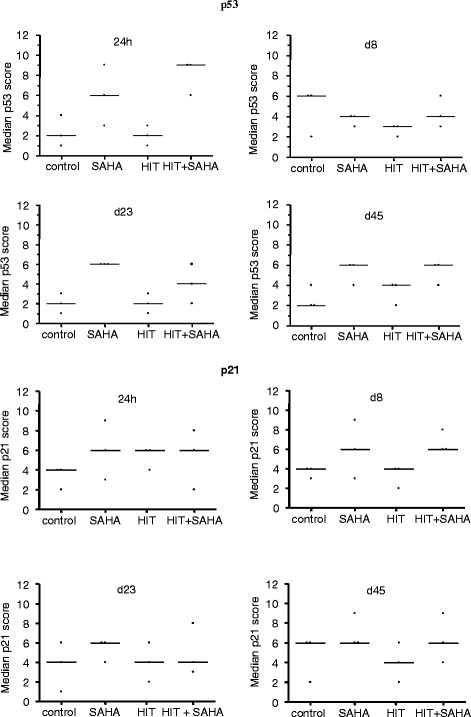
Results: Here, we show that the combination of HIT and SAHA induced a significant delay of tumor growth through increased rate of apoptosis, increased expression of p53 and p21(Waf1/Cip1), inhibition of proliferation and angiogenesis compared to tumors treated with HIT only.
Conclusion: HIT and in particular the combination of HIT and histone deacetylase inhibition is a promising treatment strategy in OS and may be tested in clinical trials.
Figures
References
-
- Schardt D, Elsässer T, Schulz-Ertner D. Heavy-ion tumor therapy: Physical and radio-biological benefits. Rev Mod Phys. 2010;82:383. doi: 10.1103/RevModPhys.82.383. - DOI
-
- Sugahara S, Kamada T, Imai R, Tsuji H, Kameda N, Okada T, et al. Carbon ion radiotherapy for localized primary sarcoma of the extremities: results of a phase I/II trial. Working group for the bone and soft tissue sarcomas. Radiother Oncol. 2012;105(2):226–31. doi: 10.1016/j.radonc.2012.09.010. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
