

Carotid intima-media thickness progression and risk of vascular events in people with diabetes: results from the PROG-IMT collaboration
- PMID: 26180107
- PMCID: PMC4580609
- DOI: 10.2337/dc14-2732
Carotid intima-media thickness progression and risk of vascular events in people with diabetes: results from the PROG-IMT collaboration
Abstract
Objective: Carotid intima-media thickness (CIMT) is a marker of subclinical organ damage and predicts cardiovascular disease (CVD) events in the general population. It has also been associated with vascular risk in people with diabetes. However, the association of CIMT change in repeated examinations with subsequent CVD events is uncertain, and its use as a surrogate end point in clinical trials is controversial. We aimed at determining the relation of CIMT change to CVD events in people with diabetes.
Research design and methods: In a comprehensive meta-analysis of individual participant data, we collated data from 3,902 adults (age 33-92 years) with type 2 diabetes from 21 population-based cohorts. We calculated the hazard ratio (HR) per standard deviation (SD) difference in mean common carotid artery intima-media thickness (CCA-IMT) or in CCA-IMT progression, both calculated from two examinations on average 3.6 years apart, for each cohort, and combined the estimates with random-effects meta-analysis.
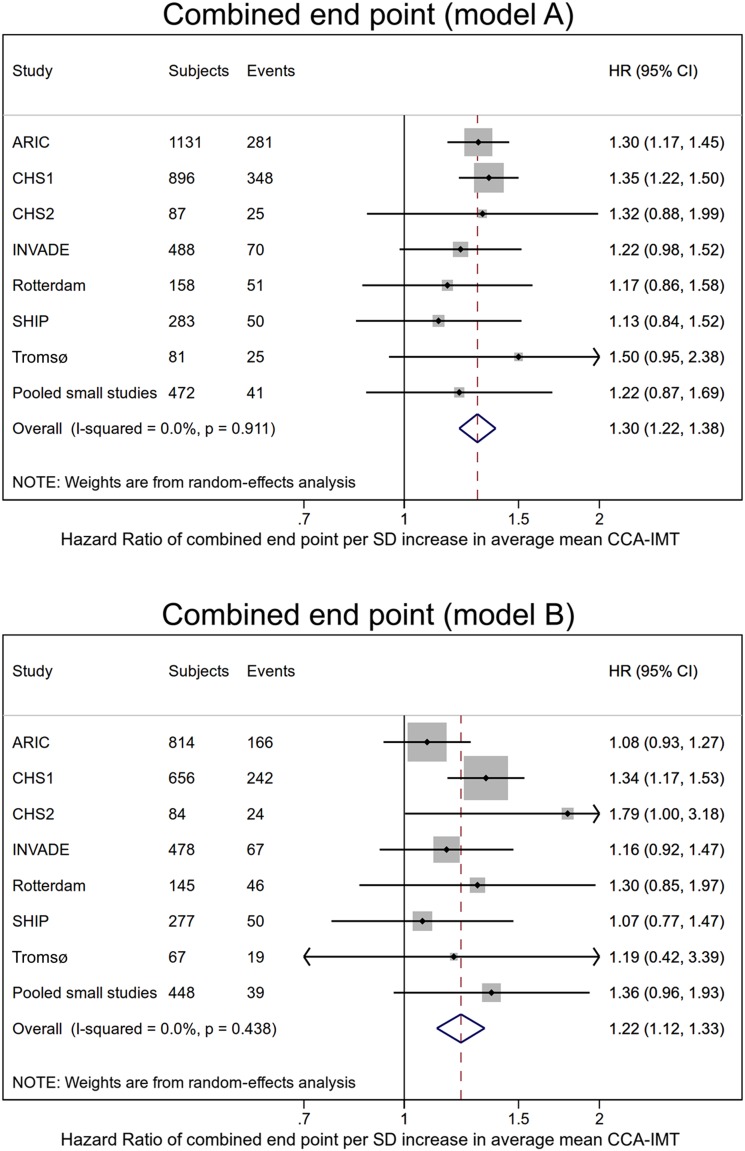
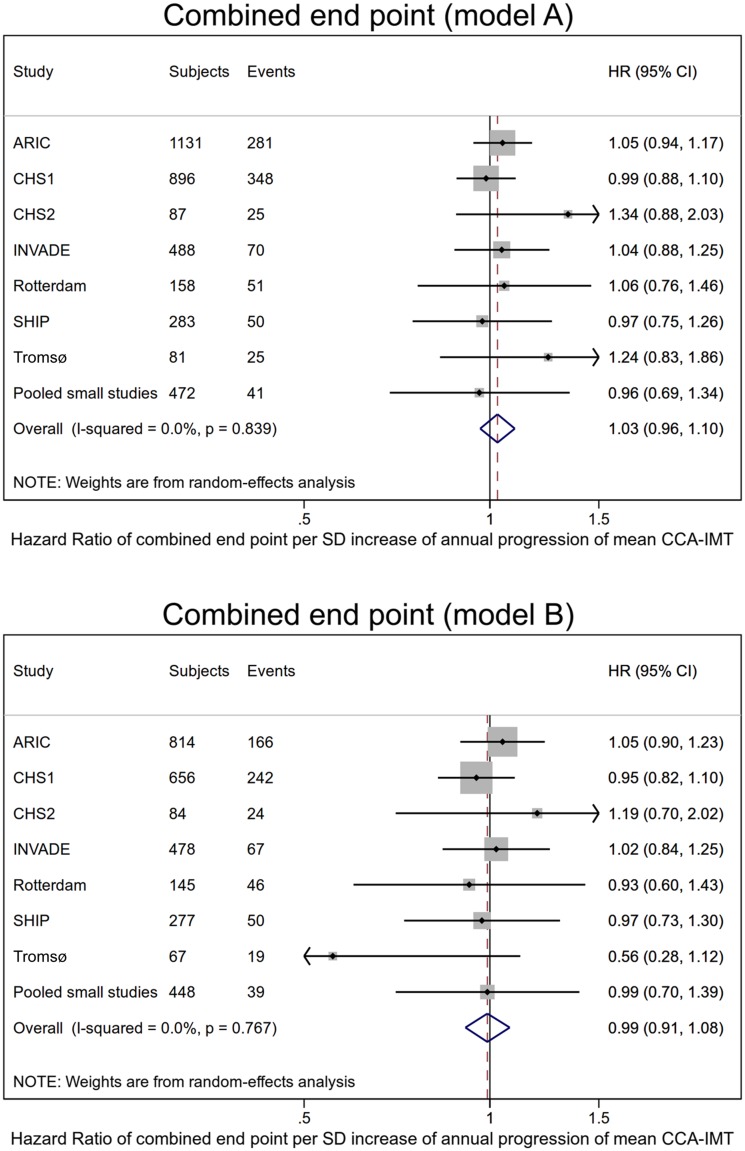
Results: Average mean CCA-IMT ranged from 0.72 to 0.97 mm across cohorts in people with diabetes. The HR of CVD events was 1.22 (95% CI 1.12-1.33) per SD difference in mean CCA-IMT, after adjustment for age, sex, and cardiometabolic risk factors. Average mean CCA-IMT progression in people with diabetes ranged between -0.09 and 0.04 mm/year. The HR per SD difference in mean CCA-IMT progression was 0.99 (0.91-1.08).
Conclusions: Despite reproducing the association between CIMT level and vascular risk in subjects with diabetes, we did not find an association between CIMT change and vascular risk. These results do not support the use of CIMT progression as a surrogate end point in clinical trials in people with diabetes.
© 2015 by the American Diabetes Association. Readers may use this article as long as the work is properly cited, the use is educational and not for profit, and the work is not altered.
Figures
References
-
- Sarwar N, Gao P, Seshasai SRK, et al.; Emerging Risk Factors Collaboration . Diabetes mellitus, fasting blood glucose concentration, and risk of vascular disease: a collaborative meta-analysis of 102 prospective studies [published correction appears in Lancet 2010;376:958]. Lancet 2010;375:2215–2222 - PMC - PubMed
-
- Woodward M, Zhang X, Barzi F, et al.; Asia Pacific Cohort Studies Collaboration . The effects of diabetes on the risks of major cardiovascular diseases and death in the Asia-Pacific region. Diabetes Care 2003;26:360–366 - PubMed
-
- Haffner SM, Lehto S, Rönnemaa T, Pyörälä K, Laakso M. Mortality from coronary heart disease in subjects with type 2 diabetes and in nondiabetic subjects with and without prior myocardial infarction. N Engl J Med 1998;339:229–234 - PubMed
-
- Wagenknecht LE, D’Agostino RB Jr, Haffner SM, Savage PJ, Rewers M. Impaired glucose tolerance, type 2 diabetes, and carotid wall thickness: the Insulin Resistance Atherosclerosis Study. Diabetes Care 1998;21:1812–1818 - PubMed
-
- Temelkova-Kurktschiev TS, Koehler C, Leonhardt W, et al. Increased intimal-medial thickness in newly detected type 2 diabetes: risk factors. Diabetes Care 1999;22:333–338 - PubMed
Publication types
MeSH terms
Grants and funding
- U01 HL080295/HL/NHLBI NIH HHS/United States
- R01 DE013094/DE/NIDCR NIH HHS/United States
- R37 NS029993/NS/NINDS NIH HHS/United States
- N01-HC-55222/HC/NHLBI NIH HHS/United States
- N01 HC085079/HL/NHLBI NIH HHS/United States
- R37-NS-029993/NS/NINDS NIH HHS/United States
- N01 HC085086/HL/NHLBI NIH HHS/United States
- RG/08/014/24067/BHF_/British Heart Foundation/United Kingdom
- U01-HL-080295/HL/NHLBI NIH HHS/United States
- R01-DE-13094/DE/NIDCR NIH HHS/United States
- MR/L003120/1/MRC_/Medical Research Council/United Kingdom
- N01-HC-85086/HC/NHLBI NIH HHS/United States
- N01-HC-15103/HC/NHLBI NIH HHS/United States
- N01 HC055222/HL/NHLBI NIH HHS/United States
- R01 NS065114/NS/NINDS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
