

Randomized Controlled Trial of Intensive Versus Conservative Glucose Control in Patients Undergoing Coronary Artery Bypass Graft Surgery: GLUCO-CABG Trial
- PMID: 26180108
- PMCID: PMC4542267
- DOI: 10.2337/dc15-0303
Randomized Controlled Trial of Intensive Versus Conservative Glucose Control in Patients Undergoing Coronary Artery Bypass Graft Surgery: GLUCO-CABG Trial
Abstract
Objective: The optimal level of glycemic control needed to improve outcomes in cardiac surgery patients remains controversial.
Research design and methods: We randomized patients with diabetes (n = 152) and without diabetes (n = 150) with hyperglycemia to an intensive glucose target of 100-140 mg/dL (n = 151) or to a conservative target of 141-180 mg/dL (n = 151) after coronary artery bypass surgery (CABG) surgery. After the intensive care unit (ICU), patients received a single treatment regimen in the hospital and 90 days postdischarge. Primary outcome was differences in a composite of complications, including mortality, wound infection, pneumonia, bacteremia, respiratory failure, acute kidney injury, and major cardiovascular events.
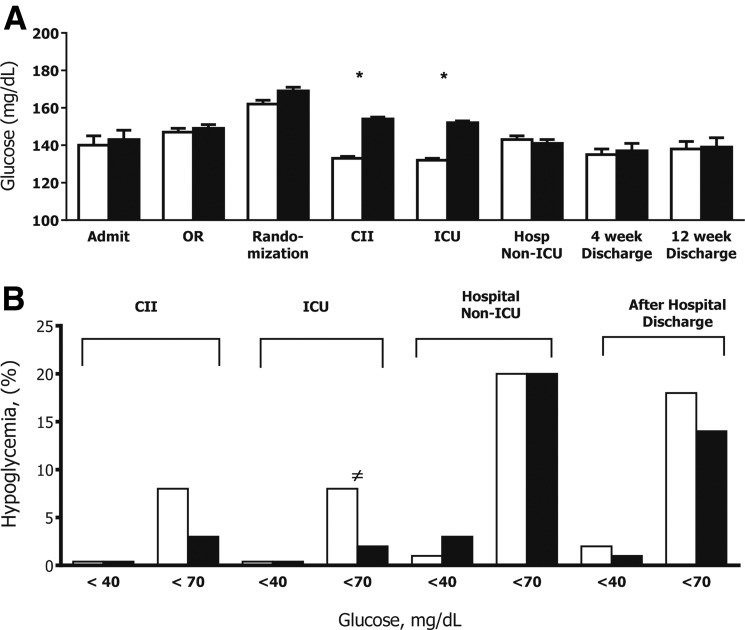
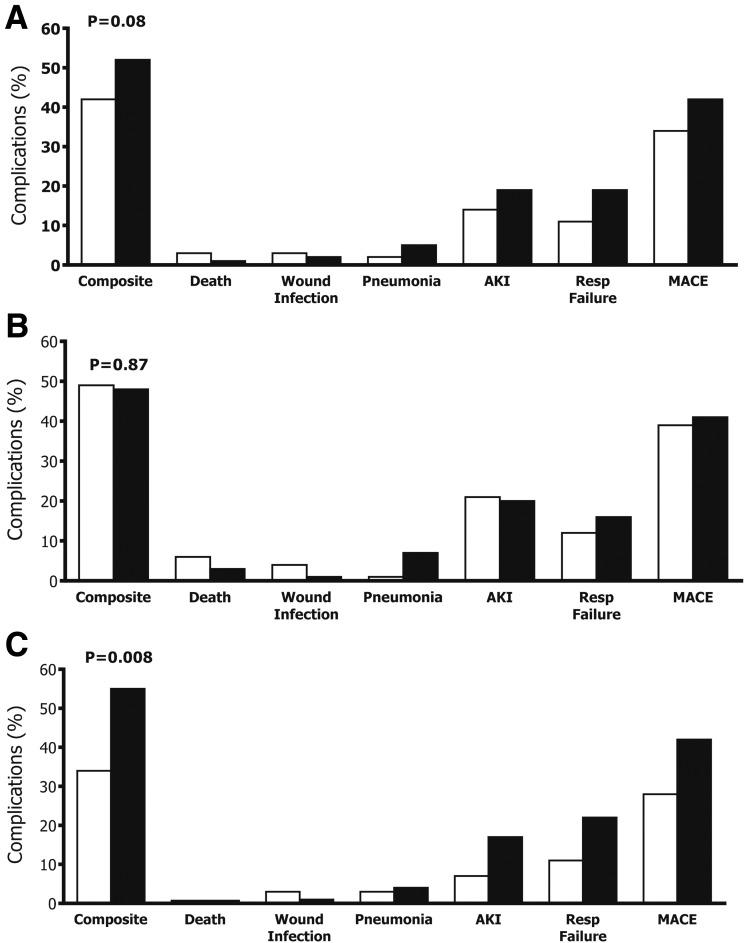
Results: Mean glucose in the ICU was 132 ± 14 mg/dL (interquartile range [IQR] 124-139) in the intensive and 154 ± 17 mg/dL (IQR 142-164) in the conservative group (P < 0.001). There were no significant differences in the composite of complications between intensive and conservative groups (42 vs. 52%, P = 0.08). We observed heterogeneity in treatment effect according to diabetes status, with no differences in complications among patients with diabetes treated with intensive or conservative regimens (49 vs. 48%, P = 0.87), but a significant lower rate of complications in patients without diabetes treated with intensive compared with conservative treatment regimen (34 vs. 55%, P = 0.008).
Conclusions: Intensive insulin therapy to target glucose of 100 and 140 mg/dL in the ICU did not significantly reduce perioperative complications compared with target glucose of 141 and 180 mg/dL after CABG surgery. Subgroup analysis showed a lower number of complications in patients without diabetes, but not in patients with diabetes treated with the intensive regimen. Large prospective randomized studies are needed to confirm these findings.
© 2015 by the American Diabetes Association. Readers may use this article as long as the work is properly cited, the use is educational and not for profit, and the work is not altered.
Figures
References
-
- McAlister FA, Man J, Bistritz L, Amad H, Tandon P. Diabetes and coronary artery bypass surgery: an examination of perioperative glycemic control and outcomes. Diabetes Care 2003;26:1518–1524 - PubMed
-
- Schmeltz LR, DeSantis AJ, Thiyagarajan V, et al. . Reduction of surgical mortality and morbidity in diabetic patients undergoing cardiac surgery with a combined intravenous and subcutaneous insulin glucose management strategy. Diabetes Care 2007;30:823–828 - PubMed
-
- Carson JL, Scholz PM, Chen AY, Peterson ED, Gold J, Schneider SH. Diabetes mellitus increases short-term mortality and morbidity in patients undergoing coronary artery bypass graft surgery. J Am Coll Cardiol 2002;40:418–423 - PubMed
-
- Furnary AP, Gao G, Grunkemeier GL, et al. . Continuous insulin infusion reduces mortality in patients with diabetes undergoing coronary artery bypass grafting. J Thorac Cardiovasc Surg 2003;125:1007–1021 - PubMed
-
- Thourani VH, Weintraub WS, Stein B, et al. . Influence of diabetes mellitus on early and late outcome after coronary artery bypass grafting. Ann Thorac Surg 1999;67:1045–1052 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
