

doi: 10.1155/2015/753160.
Epub 2015 Jun 9.
Extranodal Rosai-Dorfman Disease Involving the Left Atrium: Cardiac MRI, CT, and PET Scan Findings
Affiliations
- PMID: 26180652
- PMCID: PMC4477210
- DOI: 10.1155/2015/753160
Item in Clipboard
Extranodal Rosai-Dorfman Disease Involving the Left Atrium: Cardiac MRI, CT, and PET Scan Findings
Case Rep Radiol.
2015.
Abstract
Rosai-Dorfman disease (RDD) is a rare entity that usually involves the lymph nodes but extranodal involvements have been seen in numerous cases, although RDD with cardiovascular involvement is extremely rare. We describe a case of a young male who presented with intermittent palpitations and was found to have a left atrium mass. Our case not only emphasizes the rarity of the above lesion but also highlights the importance of modern-day imaging like computed tomography, Cardiac Magnetic Resonance Imaging (CMRI), and PET scan in characterizing such nonspecific lesions and directing appropriate line of treatment. RDD should be considered as one of the differentials even for isolated cardiac lesions.
Figures
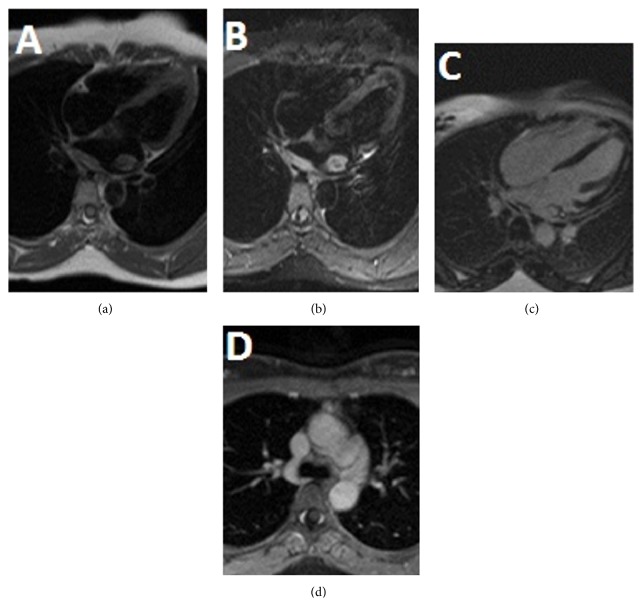
Cardiac MR (CMR) with and without contrast. T1 weighted dark blood image on 4-chamber view showed an isointense mass in left atrium with wall thickening along its posterior wall (a). Infiltrative nature of mass is noted in the form of hyperintense thickening of posterior wall of left atrium on T2 weighted dark blood image on 4-chamber view (b). Central T2 hypointensity, which is a common finding in RDD, can be seen in our case (c). Homogenous postcontrast enhancement is seen on delayed postcontrast 4-chamber view. Mediastinal lymphadenopathy with similar signal intensity as cardiac mass is seen on fat-suppressed postcontrast axial image (d). Lymphadenopathy is more marked in aortopulmonary window station.
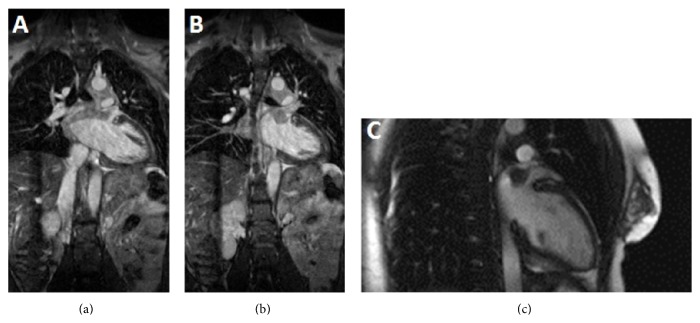
CMR—steady-state-free precession. Left atrial mass with infiltration of wall of left atrium in the form of wall thickening and postcontrast enhancement is seen on coronal steady-state-free precession images (a and b). Also seen is soft tissue mass in mediastinum with signal characteristics similar to left atrial mass. Precontrast 2-chamber view shows mass appearing isointense to left ventricular myocardium (c).
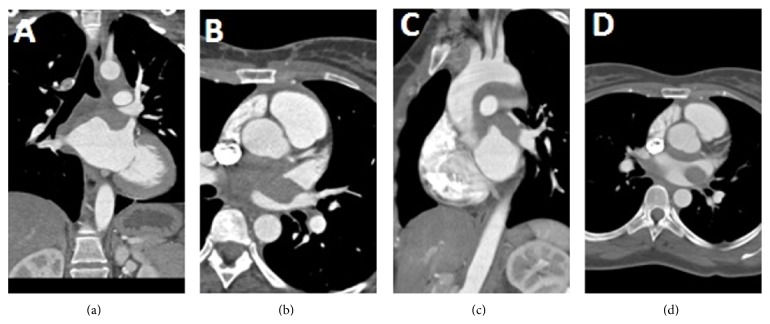
Prospectively ECG gated CT chest with contrast. Hypodense mass in left atrium is well demonstrated on coronal reconstructed images (a). CT scan helps in assessment of any possible compression of adjacent structures by mass lesion. Narrowing of left superior pulmonary vein is seen on axial image (b and d). Sagittal reconstructed image shows hypodense soft tissue thickening along the undersurface of arch of aorta that represents mediastinal lymphadenopathy (c).
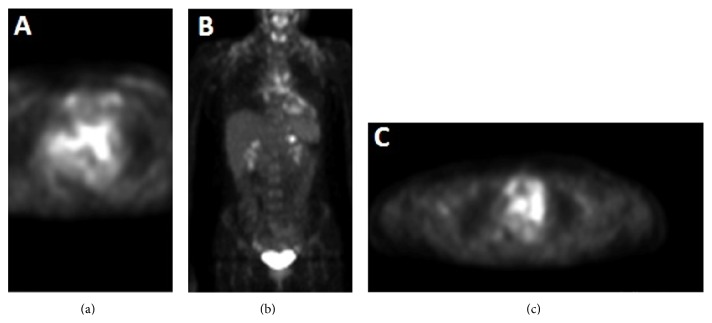
PET scan. Avid uptake of Fluorodeoxyglucose (FDG) in region of mass is seen in left atrium (a). Uptake is also seen involving mediastinal nodes. Coronal image shows uptake in cardiac mass and mediastinal nodes (b). Focal area of uptake was noted near upper pole of left kidney (c).
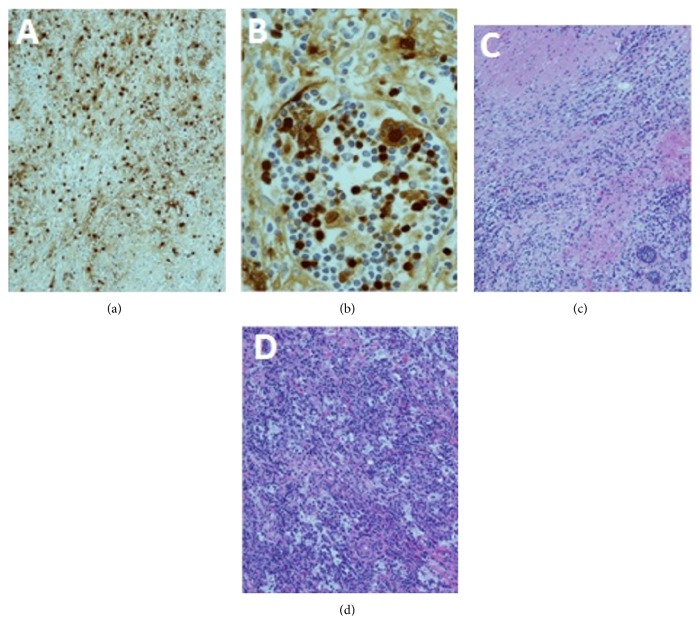
Immunohistopathology. Section through the left atrial mass shows histiocytes that are immunoreactive to S100 protein immunostaining (a). Emperipolesis is engulfment of lymphocytes and erythrocytes by histiocytes that is considered diagnostic of RDD. Emperipolesis is noted in section from left atrial mass on hematoxylin and eosin-stained sections (b). The histiocytes and lymphoplasmacytic cells infiltrating the myocardium of the left atrium are seen (c). Section from the left atrium also demonstrates fibrosis and large histiocytes in sheets that are accompanied by numerous plasma cells and small mature lymphocytes mass on hematoxylin and eosin-stained section (d).
References
-
- National Organization for Rare Disorders (NORD) Rosai-Dorfman Disease. National Organization for Rare Disorders (NORD); 2007. http://rarediseases.org/rare-diseases/rosai-dorfman-disease/
LinkOut - more resources
Full Text Sources
Other Literature Sources
