

Systemic Exposure to Thiopurines and Risk of Relapse in Children With Acute Lymphoblastic Leukemia: A Children's Oncology Group Study
- PMID: 26181173
- PMCID: PMC4561178
- DOI: 10.1001/jamaoncol.2015.0245
Systemic Exposure to Thiopurines and Risk of Relapse in Children With Acute Lymphoblastic Leukemia: A Children's Oncology Group Study
Abstract
Importance: Variability in prescribed doses of 6-mercaptopurine (6MP) and lack of adherence to a 6MP treatment regimen could result in intra-individual variability in systemic exposure to 6MP (measured as erythrocyte thioguanine nucleotide [TGN] levels) in children with acute lymphoblastic leukemia (ALL). The effect on relapse risk of this variability is unknown.
Objective: To determine the effect of high intra-individual variability of 6MP systemic exposure on relapse risk in children with ALL.
Design, setting, and participants: We used a prospective longitudinal design (Children's Oncology Group study [COG-AALL03N1]) to monitor 6MP and disease relapse in 742 children with ALL in ambulatory care settings of 94 participating institutions from May 30, 2005, to September 9, 2011. All participants met the following eligibility criteria: (1) diagnosis of ALL at 21 years or younger; (2) first continuous remission in progress at the time of study entry; (3) receiving self-, parent-, or caregiver-administered oral 6MP during maintenance therapy; and (4) completion of at least 6 months of maintenance therapy at the time of study enrollment. The median patient age at diagnosis was 5 years; 68% were boys; and 43% had National Cancer Institute-based high-risk disease.
Main outcomes and measures: Daily 6MP regimen adherence was measured over 68 716 person-days using an electronic system that recorded the date and time of each 6MP bottle opening; adherence rate was defined as the ratio of days that a 6MP bottle was opened to days thata 6MP bottle was prescribed. Average monthly 6MP dose intensity was measured over 120 439 person-days by dividing the number of 6MP doses actually prescribed by the number of planned protocol doses (75 mg/m2/d). Monthly erythrocyte TGN levels (pmol/8 × 108 erythrocytes) were measured over 6 consecutive months per patient (n = 3944 measurements). Using intra-individual coefficients of variation (CV%), patients were classified as having stable (CV% <85th percentile) vs varying (CV% ≥85th percentile) indices. Median follow-up time was 6.7 years from the time of diagnosis.
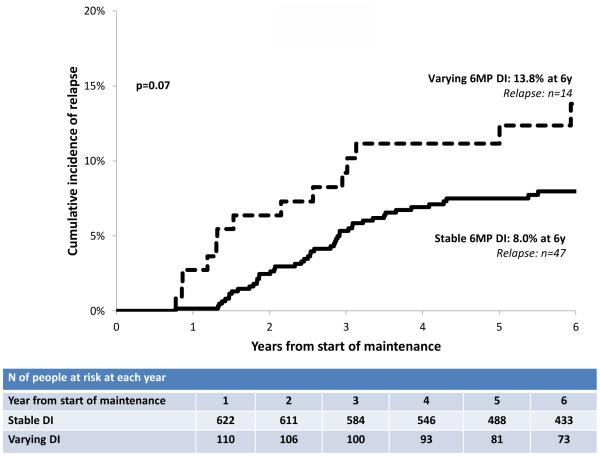
Results: Adjusting for clinical prognosticators, we found that patients with 6MP nonadherence (mean adherence rate <95%) were at a 2.7-fold increased risk of relapse (95% CI, 1.3-5.6; P = .01) compared with patients with a mean adherence rate of 95% or greater. Among adherers, high intra-individual variability in TGN levels contributed to increased relapse risk (hazard ratio, 4.4; 95% CI, 1.2-15.7; P = .02). Furthermore, adherers with varying TGN levels had varying 6MP dose intensity (odds ratio [OR], 4.5; 95% CI, 1.5-13.4; P = .01) and 6MP drug interruptions (OR, 10.2; 95% CI, 2.2-48.3; P = .003).
Conclusions and relevance: These findings emphasize the need to maximize 6MP regimen adherence and maintain steady thiopurine exposure to minimize relapse in children with ALL.
Figures




Comment in
-
Thiopurines for the Treatment of Acute Lymphoblastic Leukemia in Children: What's Old Is New.JAMA Oncol. 2015 Jun;1(3):281-2. doi: 10.1001/jamaoncol.2015.0435. JAMA Oncol. 2015. PMID: 26181170 No abstract available.
References
-
- Koren G, Ferrazini G, Sulh H, Langevin AM, Kapelushnik J, Klein J, et al. Systemic exposure to mercaptopurine as a prognostic factor in acute lymphocytic leukemia in children. N Engl J Med. 1990;323:17–21. - PubMed
-
- Karran P, Attard N. Thiopurines in current medical practice: molecular mechanisms and contributions to therapy-related cancer. Nature Rev Cancer. 2008;8:24–36. - PubMed
-
- Waters TR, Swann PF. Cytotoxic mechanism of 6-thioguanine: hMutSalpha, the human mismatch binding heterodimer, binds to DNA containing S6-methylguanine. Biochemistry. 1997;36:2501–6. - PubMed
-
- Relling MV, Hancock ML, Boyett JM, Pui CH, Evans W,E. Prognostic importance of 6-mercaptopurine dose intensity in acute lymphoblastic leukemia. Blood. 1999;93:2817–23. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- GM92666/GM/NIGMS NIH HHS/United States
- U10 CA180834/CA/NCI NIH HHS/United States
- R37 CA36401/CA/NCI NIH HHS/United States
- R01 CA096670/CA/NCI NIH HHS/United States
- CA156449/CA/NCI NIH HHS/United States
- R37 CA036401/CA/NCI NIH HHS/United States
- U10 CA095861/CA/NCI NIH HHS/United States
- RC4 CA156449/CA/NCI NIH HHS/United States
- CA21765/CA/NCI NIH HHS/United States
- UG1 CA189955/CA/NCI NIH HHS/United States
- M01 RR000043/RR/NCRR NIH HHS/United States
- U10 CA098543/CA/NCI NIH HHS/United States
- M01-RR00043/RR/NCRR NIH HHS/United States
- U10 CA180886/CA/NCI NIH HHS/United States
- U01 GM092666/GM/NIGMS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
