

Inclusion of Sarcopenia Within MELD (MELD-Sarcopenia) and the Prediction of Mortality in Patients With Cirrhosis
- PMID: 26181291
- PMCID: PMC4816259
- DOI: 10.1038/ctg.2015.31
Inclusion of Sarcopenia Within MELD (MELD-Sarcopenia) and the Prediction of Mortality in Patients With Cirrhosis
Abstract
Objectives: Limitations of the Model for End-Stage Liver Disease (MELD) score include its failure to assess the nutritional and functional status of cirrhotic patients. Our objectives were to evaluate the impact of sarcopenia in cirrhosis and whether the inclusion of muscularity assessment within MELD could improve the prediction of mortality in patients with cirrhosis.
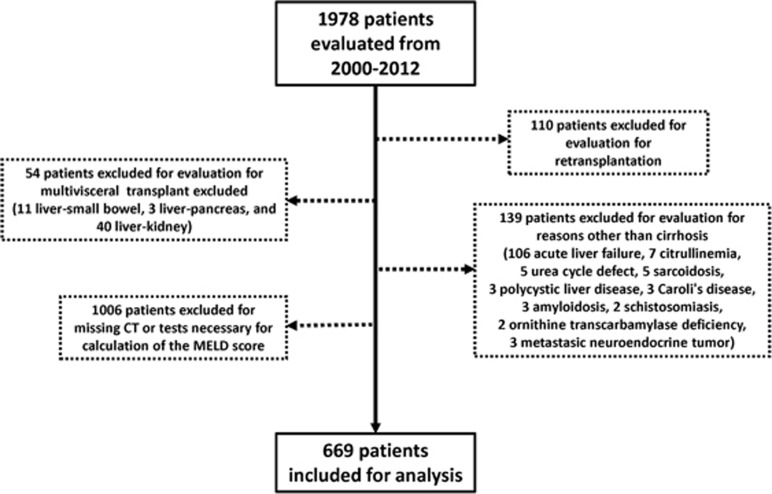
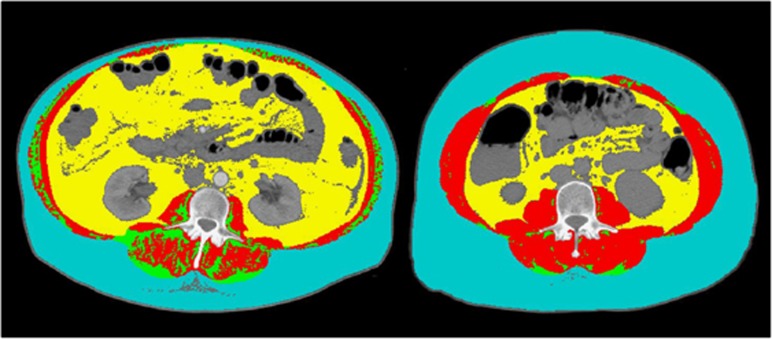
Methods: We included 669 cirrhotic patients who were consecutively evaluated for liver transplantation. Skeletal muscle index at the third lumbar vertebra (L3 SMI) was measured by computed tomography, and sarcopenia was defined using previously published gender and body mass index-specific cutoffs. Using Cox proportional hazards regression, a novel MELD-sarcopenia score was derived.
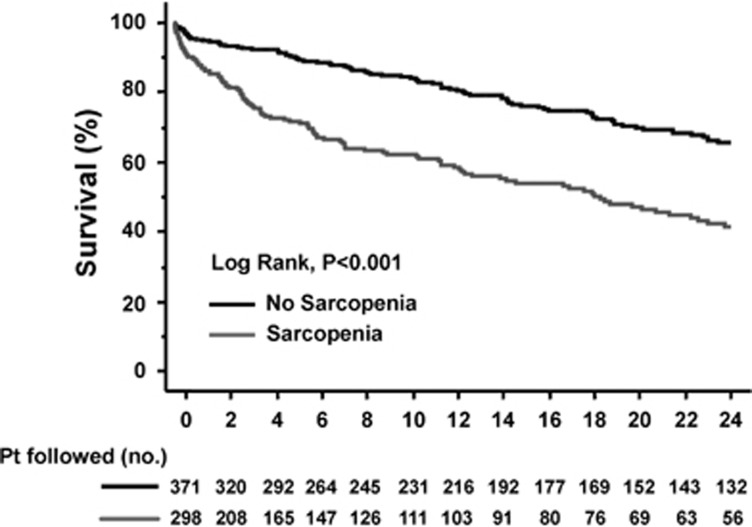
Results: Sarcopenia was present in 298 patients (45%); sarcopenic patients had shorter median survival than non-sarcopenic patients (20±3 vs. 95±24 months, P<0.001). By Cox regression analysis adjusted for age, gender, and hepatocellular carcinoma, both MELD (hazard ratio (HR) 1.08, 95% confidence interval (CI) 1.06-1.10, P<0.001), and the L3 SMI (HR 0.97, 95% CI 0.96-0.99, P<0.001) were associated with mortality. Overall, the c-statistics for 3-month mortality were 0.82 (95% CI 0.78-0.87) for MELD and 0.85 (95% CI 0.81-0.88) for MELD-sarcopenia (P=0.1). Corresponding figures for 1-year mortality were 0.73 (95% CI 0.69-0.77) and 0.77 (95% CI 0.73-0.80), respectively (P=0.03). The c-statistics for 3-month mortality in patients with MELD<15 (0.85 vs. 0.69, P=0.02) and refractory ascites (0.74 vs. 0.71, P=0.01) were significantly higher for MELD-sarcopenia compared with MELD.
Conclusions: Modification of MELD to include sarcopenia is associated with improved prediction of mortality in patients with cirrhosis, primarily in patients with low MELD scores. External validation of this prognostic index in larger cohorts of cirrhotic patients is warranted.
Figures
References
-
- Freeman RB Jr, Wiesner RH, Harper A et al. The new liver allocation system: moving toward evidence-based transplantation policy. Liver Transpl 2002; 8: 851–858. - PubMed
-
- Wiesner R, Edwards E, Freeman R et al. Model for end-stage liver disease (MELD) and allocation of donor livers. Gastroenterology 2003; 124: 91–96. - PubMed
-
- Brown RS Jr, Lake JR. The survival impact of liver transplantation in the MELD era, and the future for organ allocation and distribution. Am J Transplant 2005; 5: 203–204. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
