

Follicular Variant of Papillary Thyroid Cancer with Bilateral Renal Metastases Discovered Incidentally During Work-Up of Primary Endometrial Cancer: A Rare Occurrence
- PMID: 26181765
- PMCID: PMC4509416
- DOI: 10.12659/AJCR.894935
Follicular Variant of Papillary Thyroid Cancer with Bilateral Renal Metastases Discovered Incidentally During Work-Up of Primary Endometrial Cancer: A Rare Occurrence
Abstract
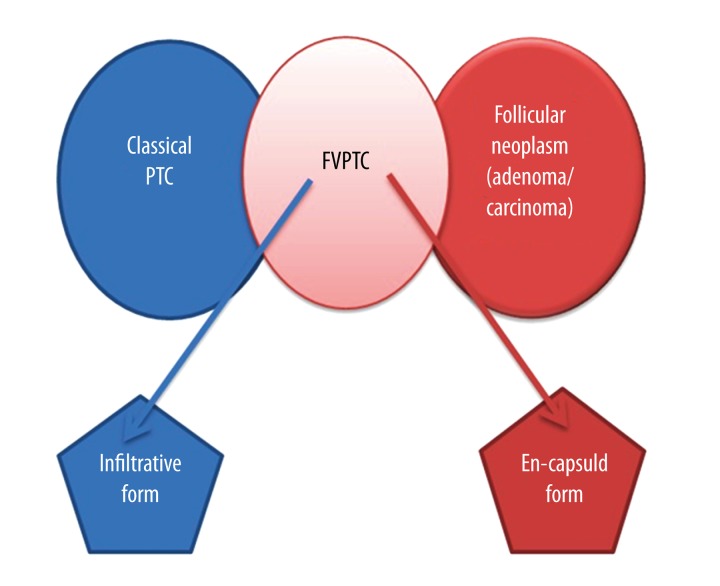
Background: Follicular variant of papillary thyroid cancer (FV-PTC) is the second most common subtype of papillary thyroid cancer (PTC) after classic PTC. FV-PTC is characterized by nuclear features consistent with classic PTC but has a follicular architecture that lacks classic papillary morphology. Thyroid cancer rarely metastasizes to the kidney. Only 6 cases of FV-PTC metastasizing to the kidney have been reported in the English literature. We are reporting a case of FV-PTC with bilateral renal metastases discovered incidentally during work-up of primary endometrial cancer.
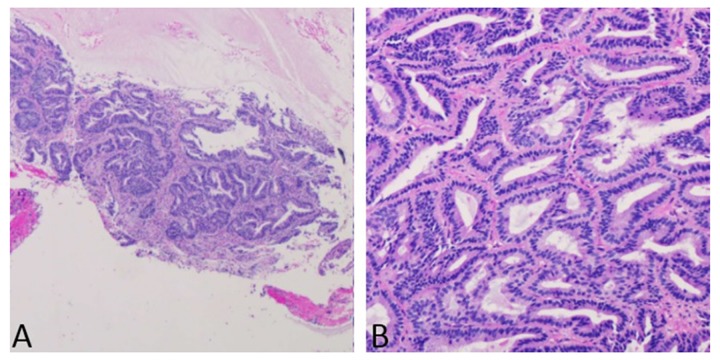
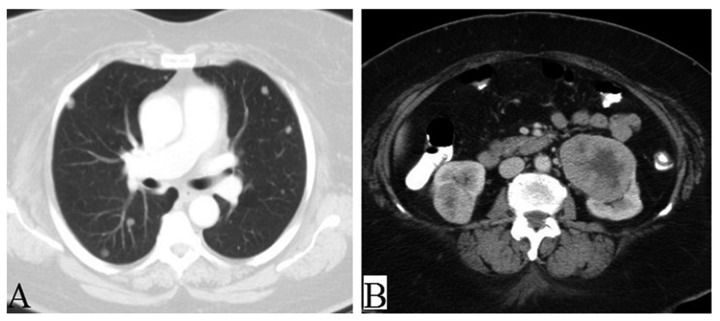
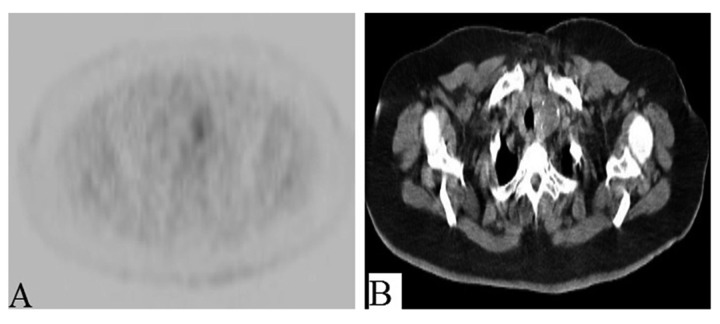
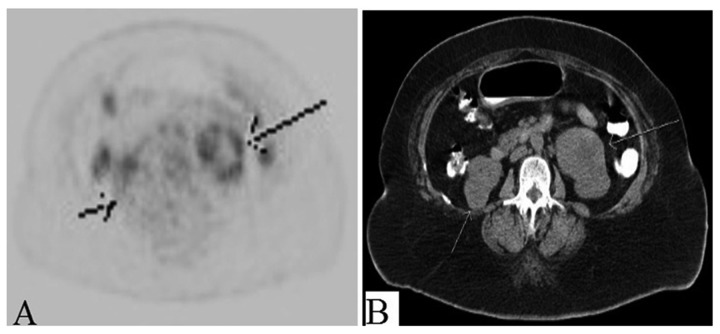
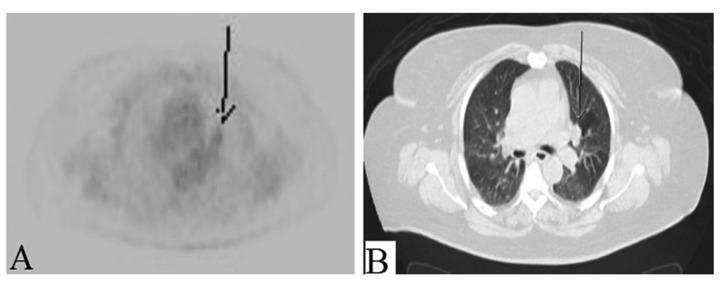
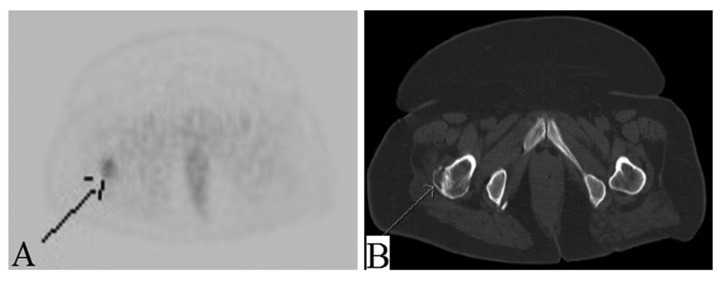
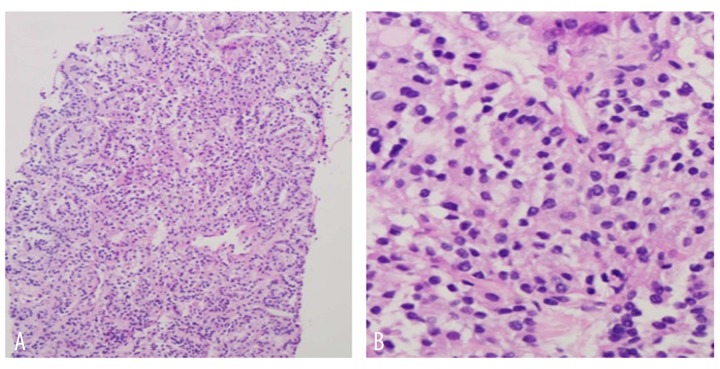
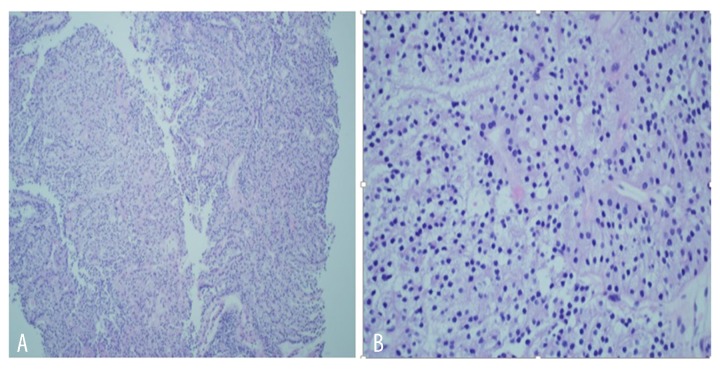
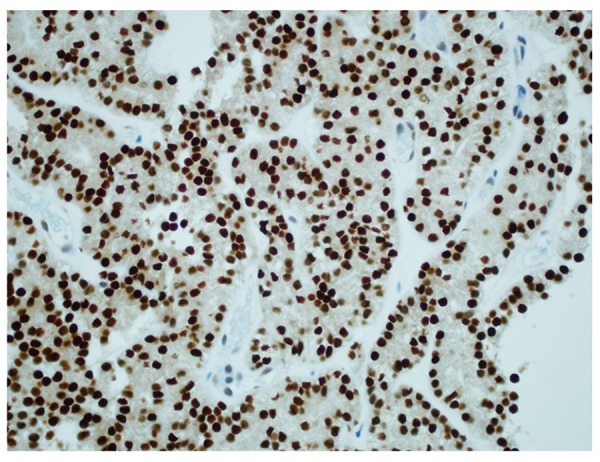
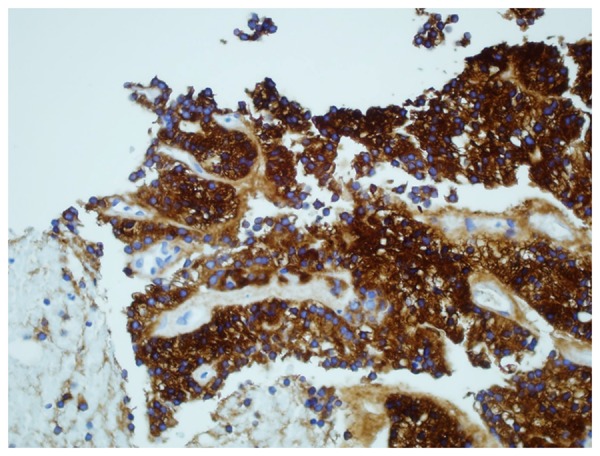
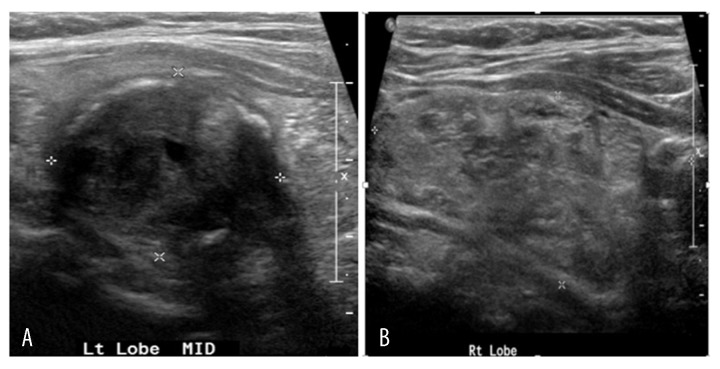
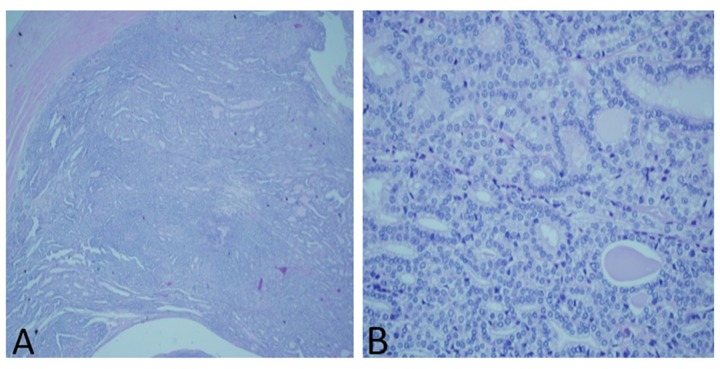
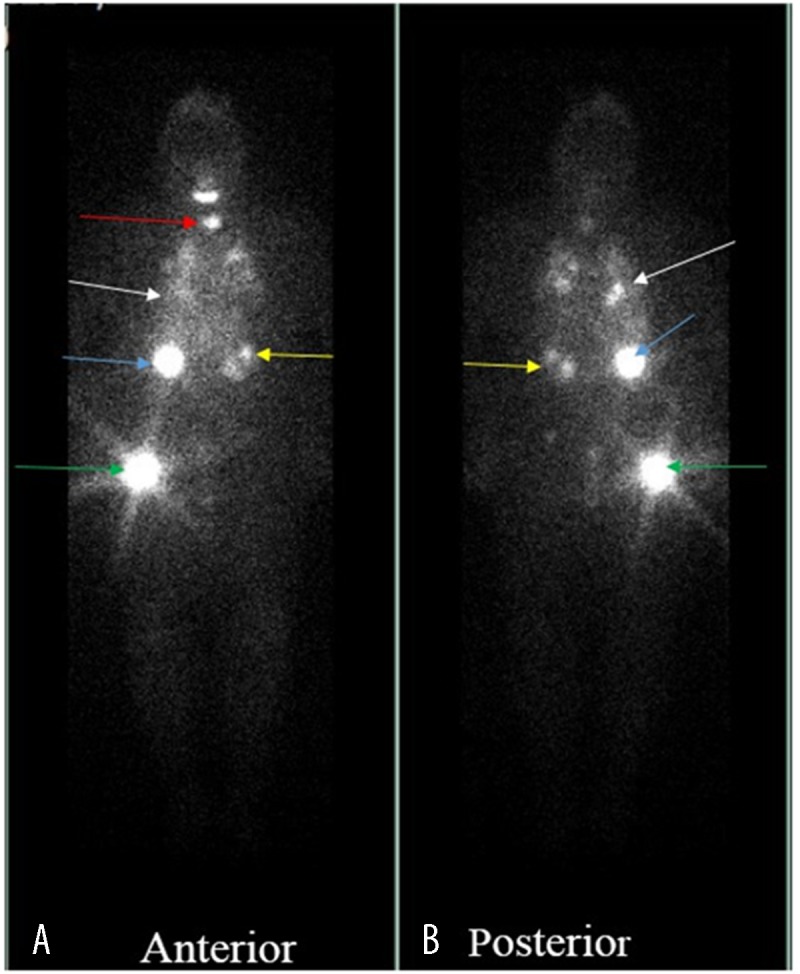
Case report: A 70-year-old woman presented with post-menopausal bleeding secondary to endometrial cancer. Staging work-up showed multiple bilateral lung nodules, bilateral soft tissue kidney masses, and multinodular goiter. The pathological and immnohistochemical profile of the lung biopsy was consistent with primary well-differentiated lung adenocarcinoma. Follow-up computerized tomography scan showed stable lung nodules and enlarging renal masses, which was suggestive of bilateral renal cancer. While the histologic features of the renal biopsy were not typical, the immunohistochemical staining of renal biopsy was positive for Paired box 8, thyroid transcription factor-1, thyroglobulin, and cytokeratin 7, suggesting the thyroid as the primary cancer site. The final histopathology on surgical specimen of total thyroidectomy revealed follicular variant of papillary thyroid cancer.
Conclusions: The presence of pulmonary nodules and kidney masses does not always suggest the lung or the kidney as primary tumor sites. The clinician should be aware of the possibility of metastasis and look for the primary source, which in the present case was FV-PTC. Immunohistochemistry plays an important role in determining the primary site of origin. In case of multiple-organ metastases, each metastatic lesion should be biopsied as soon as possible for definitive diagnosis and appropriate treatment.
Figures
References
-
- Salajegheh A, Petcu EB, Smith RA, Lam AK. Follicular variant of papillary thyroid carcinoma: a diagnostic challenge for clinicians and pathologists. Postgrad Med J. 2008;84(988):78–82. - PubMed
-
- Zhu Z, Gandhi M, Nikiforova MN, et al. Molecular profile and clinical-pathologic features of the follicular variant of papillary thyroid carcinoma. An unusually high prevalence of ras mutations. Am J Clin Pathol. 2003;120(1):71–77. - PubMed
-
- Bracken RB, Chica G, Johnson DE, Luna M. Secondary renal neoplasms: an autopsy study. South Med J. 1979;72(7):806–7. - PubMed
-
- Tur GE, Asanuma Y, Sato T, et al. Resection of metastatic thyroid carcinomas to the liver and the kidney: report of a case. Surg Today. 1994;24(9):844–48. - PubMed
-
- Graham LD, Roe SM. Metastatic papillary thyroid carcinoma presenting as a primary renal neoplasm. Am Surg. 1995;61(8):732–34. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
