

Phase II Study of Nonmyeloablative Allogeneic Bone Marrow Transplantation for B Cell Lymphoma with Post-Transplantation Rituximab and Donor Selection Based First on Non-HLA Factors
- PMID: 26183076
- PMCID: PMC4639455
- DOI: 10.1016/j.bbmt.2015.07.012
Phase II Study of Nonmyeloablative Allogeneic Bone Marrow Transplantation for B Cell Lymphoma with Post-Transplantation Rituximab and Donor Selection Based First on Non-HLA Factors
Abstract
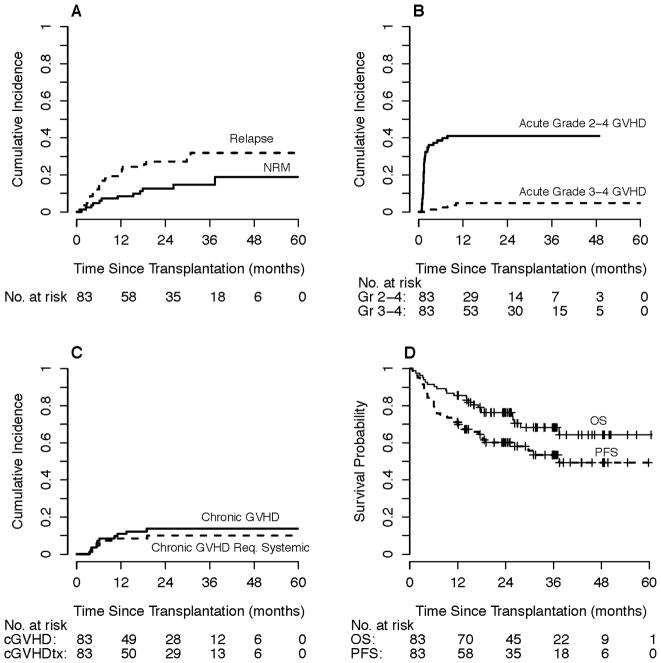
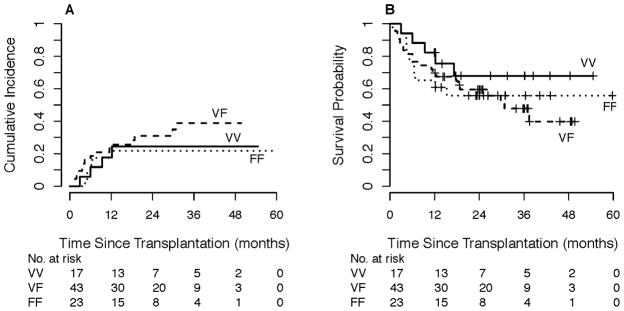
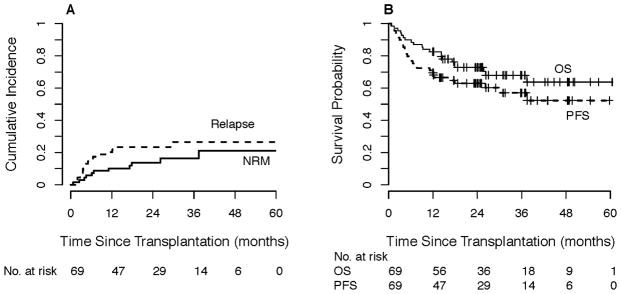
Outcomes of nonmyeloablative (NMA), HLA-haploidentical (haplo), related-donor allogeneic blood or marrow transplantation (allo-BMT) with high-dose post-transplantation cyclophosphamide (PTCy) appear to be similar to those using HLA-matched donors. Thus, it may be possible to prioritize donor factors other than HLA matching that could enhance antitumor activity. The Fc receptor polymorphism FCGR3A-158VV may confer greater sensitivity to rituximab than FCGR3A-158FF. In a prospective phase II study of NMA, related-donor allo-BMT with PTCy and post-transplantation rituximab for patients with B cell lymphomas, we hypothesized that donor selection that prioritized FCGR3A-158 polymorphism over HLA matching would be feasible, safe, and improve outcomes. The primary endpoint was 1-year progression-free survival (PFS). Of 83 patients transplanted (median age, 59 years), 69 (83%) received haplo grafts. Fifty-four (65%) received a graft that maintained or improved their Fc receptor polymorphism status. With 2.6-year median follow-up, the 1-year PFS and overall survival (OS) probabilities were 71% and 86%, respectively, with 1-year relapse and nonrelapse mortality (NRM) probabilities of 20% and 8%. At 1 year, the probability of acute grades II to IV graft-versus-host disease (GVHD) was 41%, with acute grades III to IV GVHD probability of 5% and chronic GVHD probability of 11%. Among haplo transplants, the 1-year probabilities of PFS, OS, relapse, and NRM were 70%, 83%, 20%, and 10%, respectively. No differences in outcomes were observed based on donor FCGR3A-158 polymorphism. Excess infection risk was not apparent with post-transplantation rituximab. Although donor selection based on FCGR3A-158 polymorphism was not shown to influence PFS, this study suggests that donor selection based on criteria other than best HLA match is feasible and safe. This study opens the way for the future investigation of donor prioritization based on promising non-HLA factors that may improve antitumor activity and decrease relapse after allo-BMT. This study was registered at www.clinicaltrials.gov as NCT00946023.
Keywords: Allogeneic bone marrow transplantation; Donor prioritization; Fc receptor polymorphism; Haploidentical; Post-transplantation cyclophosphamide; Post-transplantation rituximab.
Copyright © 2015 American Society for Blood and Marrow Transplantation. All rights reserved.
Figures
References
-
- Bashey A, Zhang X, Sizemore CA, et al. T-cell-replete HLA-haploidentical hematopoietic transplantation for hematologic malignancies using post-transplantation cyclophosphamide results in outcomes equivalent to those of contemporaneous HLA-matched related and unrelated donor transplantation. J Clin Oncol. 2013;31(10):1310–1316. - PubMed
-
- Burroughs LM, O’Donnell PV, Sandmaier BM, et al. Comparison of outcomes of HLA-matched related, unrelated, or HLA-haploidentical related hematopoietic cell transplantation following nonmyeloablative conditioning for relapsed or refractory Hodgkin lymphoma. Biol Blood Marrow Transplant. 2008;14(11):1279–1287. - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
