

Demographic Patterns and Outcomes of Patients in Level I Trauma Centers in Three International Trauma Systems
- PMID: 26183375
- PMCID: PMC4591196
- DOI: 10.1007/s00268-015-3162-x
Demographic Patterns and Outcomes of Patients in Level I Trauma Centers in Three International Trauma Systems
Abstract
Introduction: Trauma systems were developed to improve the care for the injured. The designation and elements comprising these systems vary across countries. In this study, we have compared the demographic patterns and patient outcomes of Level I trauma centers in three international trauma systems.
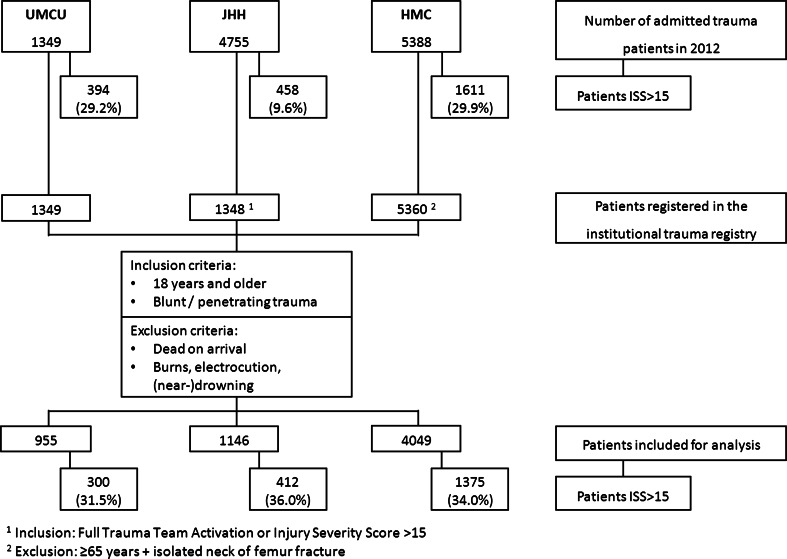
Methods: International multicenter prospective trauma registry-based study, performed in the University Medical Center Utrecht (UMCU), Utrecht, the Netherlands, John Hunter Hospital (JHH), Newcastle, Australia, and Harborview Medical Center (HMC), Seattle, the United States.
Inclusion: patients ≥18 years, admitted in 2012, registered in the institutional trauma registry.
Results: In UMCU, JHH, and HMC, respectively, 955, 1146, and 4049 patients met the inclusion criteria of which 300, 412, and 1375 patients with Injury Severity Score (ISS) > 15. Mean ISS was higher in JHH (13.5; p < 0.001) and HMC (13.4; p < 0.001) compared to UMCU (11.7). Unadjusted mortality: UMCU = 6.5 %, JHH = 3.6 %, and HMC = 4.8 %. Adjusted odds of death: JHH = 0.498 [95 % confidence interval (CI) 0.303-0.818] and HMC = 0.473 (95 % CI 0.325-0.690) compared to UMCU. HMC compared to JHH was 1.002 (95 % CI 0.664-1.514). Odds of death patients ISS > 15: JHH = 0.507 (95 % CI 0.300-0.857) and HMC = 0.451 (95 % CI 0.297-0.683) compared to UMCU. HMC = 0.931 (95 % CI 0.608-1.425) compared to JHH. TRISS analysis: UMCU: Ws = 0.787, Z = 1.31, M = 0.87; JHH, Ws = 3.583, Z = 6.7, M = 0.89; HMC, Ws = 3.902, Z = 14.6, M = 0.84.
Conclusion: This study demonstrated substantial differences across centers in patient characteristics and mortality, mainly of neurological cause. Future research must investigate whether the outcome differences remain with nonfatal and long-term outcomes. Furthermore, we must focus on the development of a more valid method to compare systems.
Figures
References
-
- American College of Surgeons Committee on Trauma . Resources for optimal care of the injured patient 2006. Chicago: American College of Surgeons; 2006.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
